Pharmacophore an International Research Journal
Awareness of Medical Staff for Vein Saving in The Patient with CKD In King Abdul-Aziz Specialist Hospital, King Faisal Hospital and Armed Forces Hospital, Taif City, Saudi Arabia
Faisal Khaled H Alhomayani1*, Nada Eidhah Algethami2, Ghaida Hassan Alotaibi2, Rahma Abdullah Algethami2, Nouran Khalid Althumali2, Raghad Sami Aljuaid2
|
|
|
ABSTRACT
Background: Hemodialysis is an essential life-protection strategy in patients with acute kidney injury (AKI) and chronic kidney illness. Between 25% of patients making dialysis using catheters in the first to start with which are invariably removed in patients with AKI. While in the setting of AKI inception of hemodialysis through a catheter is logical to continuation with in Chronic Renal disease patients catheter use must be limited to keep away from its complication. there is consistently reluctance among CKD patients for experiencing arteriovenous (AV) fistula, so the catheter stays in situ for a more extended time in certain patients. This features the need for Individuals awareness among Chronic Renal disease patients. Also, the weak of vascular tree avoid the formation of AV fistula in few CKD patients. For this should be aware of the clinical group for Vein protection in the patient with CKD in Saudi Arabia CKD patients and their doctors should know about possible expected to veins protection and important in the event a new access entrance is required. Aim of the study: To determine the awareness of medical staff for vein saving in the patient with CKD in King Abdul-Aziz Specialist Hospital, King Faisal Hospital, and Armed Forces Hospital, Taif city, KSA. Method: Cross-sectional study will be conducted to determine the awareness of medical staff for vein saving in the patient with CKD in Taif hospitals our total participants were 315 medical staff (doctor, nurses). Results: level of awareness about Patient with history of CKD our study shows that is significant relationship between the Score the level of awareness was the p-value <0.001and Chi-square (X2 -125.19) while ranging were ( 0-6) and Mean± SD (2.041±1.428 ) and the most of participants (47.0%) have Weak awareness about Patient with history of CKD followed by high awareness were (5.1%). Conclusions: Levels of awareness and knowledge among providers must be improved to prevent CKD, its progression, and the vein saving in the patient with CKD. More research is needed to awareness of medical staff for vein saving in the patient with CKD in Saudi Arabia.
Keywords: Awareness, medical staff, vein, saving, patient, CKD, Taif city, Saudi Arabia.
Introduction
Chronic kidney disease (CKD) is a typical and developing issue around the world; in the United States, >10% of adults displaying proof the harm in kidney and/or decreased kidney work [1]. Distinguishing CKD requires knowledge of individual perils and proper laboratory testing (serum creatinine as well as urinary protein) [2]. Chronic kidney disease (CKD) is a rising community health issue characterized as variations from the norm of kidney structure or capacity introduced for>3 months [1, 2]. In the Kingdom of Saudi Arabia (KSA), CKD is assessed to influence roughly 1.72 million Saudis [3]. It is roughly comparing 6% of the populace. When CKD progress to end-stage renal illness, it need dialysis treatment [1]. In KSA the occurrence of dialysis changed into 136 new cases for each million populaces [4]. The insurance of veins during the earlier phases of CKD is pivotal for the achievement of vascular access [5]. Moreover, the vast majority with the illness, particularly preceding ESRD, stay ignorant of their illness [6, 7]. Awareness for vein assurance in the patient with CKD remains unsuitably low, regardless on going endeavors to expand awareness through dissemination of clinical practice rules and proposals for patients with CKD or its hazard factors to caregiver [8, 9], public awareness occasions, for example, World Kidney Day [10, 11]. Central venous catheters are connected to a 15-fold extended hazard risk for septicemia in contrast with the AV fistula. [12] Moreover, it is exceptionally connected to morbidity, also to the raised danger of infective endocarditis. [13] There is a 10% expanded danger of mortality with CRBSI. The information from France suggests that there is a general frequency of colonization of 38.9 and bloodstream contamination disease of 1.9/1000 catheter-days. [6] The process of CRBSI can be avoided by assuming stringent infection control measures and procedures. [14]. Also, many identified behaviors to reach this aim like early transfer of CKD patients to nephrologists before the beginning of hemodialysis to allow enough time the construction of AV access, trained access surgeon working as a part of vascular access team and veins saving. The Association for Vascular Access (AVA) and the American Society of Diagnostic and Interventional Nephrology (ASDIN) understood the significance of vein assurance in chronic kidney illness patients [15]. Up to our knowledge, there are very few studies have been performed to assess awareness of the importance of vein saving in patients with chronic kidney disease among medical staff. In this study; we will evaluate the knowledge of the medical staff to protect the vein in patients with CKD in our city (Taif) as there is no study in the literature about it in Taif.
The burden of the common chronic, preventable disease and their serious outcomes make the determine awareness of medical staff vein saving in the patient with CKD topic enormously essential. Up to our knowledge, there are very little examination has been performed to assess the attention to the significance of vein saving in patients with chronic kidney disease among medical staff. This research will evaluate the knowledge of the medical staff to protect the vein in patients with CKD in our city (Taif) as there is no study in the literature about it in Taif. Thus investing in this topic well fulfills the researcher's aim.
Rationale
There are very few studies have been performed to assess awareness of the importance of vein saving in patients with chronic kidney disease among medical staff. The decided attention to clinical staff vein-protect in the patient with CKD subject is hugely important. In this study; we will evaluate the knowledge of the medical staff to protect the vein in patients with CKD in our city (Taif) as there is no study in the literature about it in Taif.
Aim of the study:
To determine the awareness of medical staff for vein saving in the patient with CKD in King Abdul-Aziz Specialist Hospital, King Faisal Hospital, and Armed Forces Hospital, Taif city, Saudi Arabia.
Objectives:
Methodology
Study Design:
A cross-sectional study will be showed to determine awareness of clinical staff for vein saving in the patient with CKD in Taif hospitals
Study Area:
This study has been conducted in Taif hospitals, which has a large number of different nationalities and different cultures. Out of these, in King Abdul-Aziz Specialist Hospital, King Faisal Hospital, and Armed Forces Hospital, Taif city, Saudi Arabia. Where the researcher has been conducted the research after all medical staff (physicians and nurses) caring for patients with CKD has been contacted during the study duration between medical staff.
Study Population:
This study has towards all medical staff (physicians and nurses) caring patients with CKD will.
Inclusion criteria:
Exclusion Criteria:
Sample Size:
The researcher has used 50%, moreover, based upon a confidence level of 95% and margin of error of 5%. The sample size calculated using the Raosoft calculator will be 315 medical staff (physicians and nurses), which increased by 10% to overcome the non-respondents.
Sampling Technique:
The researcher has used simple randomization between all medical staff (physicians and nurses) caring for patients with CKD.
Has been contacted during the study duration between medical staff to cover the sample size.
Data Collection Tool:
The researcher has used a self-administrated questionnaire. The questionnaire has included; socio-demographic data, a checklist about the level of the awareness of medical staff for vein saving in the patient with CKD. The researcher has constructed and has put the questionnaire between the hands of Scientific Research Center Research Ethics Committee consultants for validation.
Data Collection technique:
The researcher has been distributed the questionnaire personally to all medical staff (physicians and nurses) caring for patients with CKD in the division after approval from higher authorities acquired, during the working hours, specifically between the break time. Where a short introduction about the research and its importance was introduced. Afterward, the researcher has handled the questionnaire to the available medical staff (physicians and nurses) at the department. The response rate was high.
Study variables:
Data Entry and Analysis:
The researcher has used the statistical program for social sciences SPSS software 23.0 for data entry and analysis. Statistical tests such as Chi-square T-test and other appropriate tests had been used. A p-value of less than 0.05 has been adopted for statistical significance.
Pilot Study/Pretesting:
The questionnaire has been applied to 10% of the sample size over the medical staff which has dealt with the patient with chronic kidney disease in Taif city.
Scientific Research Consideration :
Relevance & expectations:
Budget
Self-funded study.
Result
Response rate:
The study included 315 medical staff in King Abdul-Aziz Specialist Hospital, King Faisal Hospital, and Armed Forces Hospital, Taif city, Saudi Arabia follow up and were enrolled in this study.
Table (1): The Describe of demographic information in participants.
|
N |
% |
|
|
Age |
||
|
<25 |
22 |
7.0 |
|
25-29 |
120 |
38.1 |
|
30-35 |
97 |
30.8 |
|
35-40 |
42 |
13.3 |
|
40-50 |
13 |
4.1 |
|
>50 |
21 |
6.7 |
|
Sex |
||
|
Female |
189 |
60.0 |
|
Male |
126 |
40.0 |
|
Working years |
||
|
<5 |
141 |
44.8 |
|
5-10 |
105 |
33.3 |
|
>10 |
69 |
21.9 |
|
Job title |
||
|
Medical doctor |
144 |
45.7 |
|
Nurse |
171 |
54.3 |
|
Institute |
||
|
King Abdul Aziz Specialist hospital |
105 |
33.3 |
|
King Faisal Medical Hospital |
76 |
24.1 |
|
Alhada Armed Forces Hospital |
111 |
35.2 |
|
Other |
23 |
7.3 |
Regarding the age majority of the study groups participants have been in the period variety of (25-29) ages in the rate of (38.1%) while participant staff were in the age, (30-35) were (30.8%).
Regarding the sex, many of the respondents were female (60.0%), male were (40.0%)
Regarding the working years, the majority of respondents have experience duration (5-10) had (33.3 (
Regarding the job title, the majority participant were nurse (54.3) but a medical doctor were (45.7 %(
Regarding the institute, many of the respondents were in Alhada Armed Forces Hospital (35.2%) while King Abdul Aziz Specialist hospital were (33.3%) while King Faisal Medical Hospital were (24.1) while other were (7.3).
Table (2) Description the general awareness of the participants ( medical staff ) for vein saving in the patient with CKD
|
N |
% |
|
|
Do you think a vein preserve is important to renal patients? |
||
|
Yes |
284 |
90.2 |
|
No |
9 |
2.9 |
|
I don't know |
22 |
7.0 |
|
Why vein preserve is important in renal disease patients? |
||
|
To avoid infection. |
56 |
17.8 |
|
Possible AV fistula creation in future |
212 |
67.3 |
|
To avoid bleeding |
19 |
6.0 |
|
I do not know |
28 |
8.9 |
|
Do you have a vein saving protocol for renal disease patients at risk in your institute? |
||
|
Yes |
175 |
55.6 |
|
No |
40 |
12.7 |
|
I don't know |
100 |
31.7 |
|
If you answered yes, to the previous question, how often do you follow this protocol |
||
|
All the time |
80 |
45.7 |
|
Most of the time |
37 |
21.1 |
|
Some time |
38 |
21.7 |
|
Rarely |
3 |
1.7 |
|
Never |
17 |
9.7 |
|
How to recognize renal disease patients who require vein preservation protocol? |
||
|
By creatinine level |
117 |
37.1 |
|
By GFR (Glomerular Filtration Rate) |
117 |
37.1 |
|
Family history of renal disease |
29 |
9.2 |
|
I don't know |
52 |
16.5 |
|
At which stage of chronic kidney disease patients needs vein preservation protocol? |
||
|
Starting from stage 1 |
66 |
21.0 |
|
Starting from stage 2 |
27 |
8.6 |
|
Starting from stage 3 |
60 |
19.0 |
|
starting from stage 4 |
54 |
17.1 |
|
Only after hemodialysis initiation |
38 |
12.1 |
|
I don't know |
70 |
22.2 |
In the table 2 show whether a vein preserve is important to renal patients most the participants answer yes the percentage were (90.2%) while participant answer I don't know the percentage were (7.0%)
Regarding Why vein preserve is important in renal disease patient majority of the study groups answer Possible AV fistula creation future the percentage were (67.3 %) while to avoid infection the percentage were (17.8 %), While the correct answer was to avoid bleeding percentage were (6.0%) while answer I do not know percentage were (8.9 %).
Regarding you have a vein saving protocol for renal disease patients at risk in your institute the majority of participants answer yes the percentage were (55.6%) followed by I don't know percentage were (31.7%) while participant answer No (12.7%)
Regarding how often do you follow this protocol majority of the study groups answer all the time participants answer (45.7%) while some time participants were (21.7%) but answer most of the time were (21.1%) and the responses never were (9.7%) while answer rarely were (1.7%)
As to conclusion of renal sickness patients who require vein safeguarding convention, the greater part of the study groups answered wrong answers by creatinine level (37.1%) followed by I don't know (16.5%) family history of renal disease (9.2%)while the correct answer is by GFR (Glomerular Filtration Rate) their percentage (37.1%).
Regarding which stage of chronic kidney disease patients needs vein preservation protocol majority of the study groups answered wrong starting from stage 1were (21.0%) while starting from stage 3 were (19.0%) but the only after hemod were (8.6%) while the correct answer the starting from stage 4 were (17.1%).
Table (3) Description the general awareness the participants about know other targeted teams for vein saving in the patient with CKD.
|
N |
% |
|
|
Do you know other targeted groups (renal disease group) for vein saving? |
||
|
Yes |
157 |
49.8 |
|
No |
158 |
50.2 |
|
If you answered yes the previous question, what is/are the targeted group? |
||
|
Functional kidney transplant |
30 |
14.65 |
|
Patient with history of recurrent kidney stones |
21 |
13.38 |
|
Patients on dialysis (HD or PD) |
117 |
74.52 |
|
Previous history of kidney biopsy-proven acute interstitial nephritis (currently preserved kidney function) |
45 |
28.66 |
Regarding you know other targeted teams (renal disease group) for vein saving the most of participants answer No the percentage were (50.2%) followed by answer yes the percentage were (49.8%).
Regarding what is/are the targeted group majority of the study groups answered correct functional kidney transplant were (14.65% ) and also correct answer patients on dialysis (HD or PD) were (74.52%) while
Answered wrong Previous history of kidney biopsy-demonstrated acute were interstitial nephritis (currently preserved kidney function) were(28.66%) followed by also answered wrong and answered wrong also wrong and replied mistakenly additionally affected person with presence of repeated kidney pebbles were (13.38%).
Table (4) Description the awareness of the participants about educates Patient with history of recurrent kidney stones.
|
N |
% |
|
|
Do you educate renal disease patients at risk or check their knowledge about the importance to save veins during the medical evaluation? |
||
|
Yes |
166 |
52.7 |
|
No |
61 |
19.4 |
|
I don't know |
88 |
27.9 |
|
Do you use instruction or warning methods (like labels, written paper instructions..etc. ) to reinforce vein saving in those risky renal disease patients? |
||
|
Yes |
146 |
46.3 |
|
No |
108 |
34.3 |
|
I don't know |
61 |
19.4 |
|
What is the primary site for venipuncture when you obtain blood samples from patients at risk? |
||
|
Dorsum of the dominant hand |
50 |
15.9 |
|
Dorsum of the non-dominant hand |
67 |
21.3 |
|
Antecubital fossa of the dominant side |
39 |
12.4 |
|
Antecubital fossa of the non-dominant side |
65 |
20.6 |
|
I do not know |
94 |
29.8 |
|
For patients with AV fistula, Do you Procedure the fistula limb for venipuncture or an IV infusion or arterial mark? |
||
|
Yes |
47 |
14.9 |
|
No |
213 |
67.6 |
|
I don't know |
55 |
17.5 |
|
If the participant needs an indwelling catheter for domestic antibiotics or different therapy, do you insertion or order to insert a small bore (<8 French)? |
||
|
Yes |
74 |
23.5 |
|
No |
133 |
42.2 |
|
I don't know |
108 |
34.3 |
|
What is the primary site for venipuncture when you obtain blood samples from those patients? |
||
|
Dorsum of the fistula site |
27 |
8.6 |
|
Dorsum of the non-fistula site |
111 |
35.2 |
|
Antecubital fossa of the fistula site |
22 |
7.0 |
|
Antecubital fossa of the non-fistula site |
68 |
21.6 |
|
I do not know |
87 |
27.6 |
|
If a patient requires an IV catheter for medications, do you insert or order to insert a small-bore size (<8 French)? |
||
|
Yes |
93 |
29.5 |
|
No |
121 |
38.4 |
|
I don't know |
101 |
32.1 |
|
Do you need the fistula limb for venipuncture or an IV infusion or arterial mark? |
||
|
Yes |
47 |
14.9 |
|
No |
199 |
63.2 |
|
I don't know |
69 |
21.9 |
|
for patients with AV fistula, Do you Use the fistula limb for blood pressure measurement? |
||
|
Yes |
36 |
11.4 |
|
No |
212 |
67.3 |
|
I don't know |
67 |
21.3 |
In the table 4 show you educate renal disease patients at risk or check their knowledge about the importance to save vein during medical evaluation the most of participants answer yes the percentage were (52.7% ) followed by I don't know percentage were (27.9% )while participant answer No (19.4%)
Regarding you instruction or warning methods (like labels, written paper instructions..etc. ) to reinforce vein saving in those risky renal disease patient the most of participants answer yes the percentage were (46.3 % ) while participant answer No (34.3%) followed by I don't know percentage were (19.4% )
What is the primary site for venipuncture when you obtain blood samples from patients at risk.
Regarding the primary site for venipuncture when you obtain blood samples from patients at risk the participants answered correct Dorsum of the dominant hand percentage were (15.9 %) followed by I don't know percentage were (29.8%) while answered wrong Dorsum of the non-dominant hand, Antecubital fossa of the non-dominant side and Antecubital fossa of the dominant side the percentage Respectively were (21.3 %, 20.6%, 12.4%)
Regarding patients with AV fistula, Do you need fistula limb for venipuncture or IV infusion or arterial mark, most the participants answer No the percentage were (67.6%) followed by I don't know percentage were (17.5 %)while participant answer yes (14.9%)
Regarding If a patient requires an indwelling catheter for home antibiotics or other medications, do you insert or order to insert a small bore (<8 French), most of the participants that answered No were (42.2 %), followed by I don't know were (34.3 %),while participants answered yes were (23.5 %)
If an affected person has an operating HD entree (fistula or graft)
the primary site venipuncture when obtain blood samples from patients, percentage the participants answered correctly for dorsum of the non-fistula site were(35.2 %) followed I don't know (27.6%)but percentage the ones answered incorrectly for Antecubital fossa of the non-fistula site, dorsum the fistula site and Antecubital fossa of the fistula site Respectively were (21.6 %, 8.6%, 27.6%), patient requires an IV catheter for medications, you insert or order to insert a small-bore size (<8 French), the percentage most the participants that answered No were (38.4 %) followed I don't know (32.1 %)while participant that answered yes were (29.5 %)
Regarding need fistula limb for venipuncture or an IV infusion or arterial line most the participants answer No percentage were (63.2%) followed by I don't know (21.9%) while participants answered yes were (14.9%), patients with AV fistula, Do you Use the fistula limb for blood pressure measurement, percentage most participants answered No were (67.3%) followed by I don't know (21.3%) while participant answered yes were (11.4%)
Table (5) Description the Level of awareness
|
Level of awareness |
Score |
||||
|
N |
% |
Range |
Mean± SD |
||
|
No |
52 |
16.5 |
0-6 |
2.041±1.428 |
|
|
Weak |
148 |
47.0 |
|||
|
Average |
99 |
31.4 |
|||
|
High |
16 |
5.1 |
|||
|
Total |
315 |
100.0 |
|||
|
Chi-square |
X2 |
125.19 |
|||
|
P-value |
<0.001* |
||||
In the table (5) and figure (1) shows level of awareness about Patient history of CKD our study shows that a significant relationship between the Score the level of awareness was the p-value <0.001and Chi-square (X2=125.19) while ranging were (0-6) and Mean±SD (2.041±1.428) and the most participants (47.0%) have Weak awareness about Patient with history of CKD While Among' Average,' the participants were (31.4%), While No awareness were (16.5%) followed by high awareness were (5.1%)
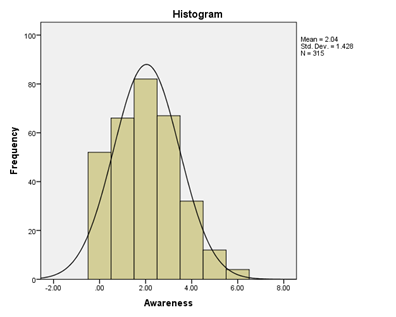
Figure (1): Histogram with normal curve description level of awareness and frequency
Table (6) Describe the relation of the Demographic data (age, six, working years, job title, and institute) and Awareness about Patient with a history of CKD
|
Demographic data |
N |
Awareness |
ANOVA or T-test |
||||
|
Mean |
± |
SD |
Test value |
P-value |
|||
|
Age |
<25 |
22 |
1.773 |
± |
1.193 |
2.249f |
0.049* |
|
25-29 |
120 |
1.867 |
± |
1.328 |
|||
|
30-35 |
97 |
1.969 |
± |
1.388 |
|||
|
35-40 |
42 |
2.429 |
± |
1.595 |
|||
|
40-50 |
13 |
2.308 |
± |
1.797 |
|||
|
>50 |
21 |
2.714 |
± |
1.586 |
|||
|
Sex |
Female |
189 |
1.963 |
± |
1.330 |
-1.155t |
0.249 |
|
Male |
126 |
2.159 |
± |
1.562 |
|||
|
Working years |
<5 |
141 |
1.745 |
± |
1.386 |
9.882f |
<0.001* |
|
5-10 |
105 |
2.038 |
± |
1.330 |
|||
|
>10 |
69 |
2.652 |
± |
1.483 |
|||
|
Job title |
Medical doctor |
144 |
2.194 |
± |
1.657 |
1.705t |
0.089 |
|
Nurse |
171 |
1.912 |
± |
1.192 |
|||
|
Institute |
King Abdul Aziz Specialist hospital |
105 |
2.029 |
± |
1.638 |
0.508f |
0.677 |
|
King Faisal Medical Hospital |
76 |
2.197 |
± |
1.386 |
|||
|
Alhada Armed Forces Hospital |
111 |
1.937 |
± |
1.223 |
|||
|
Other |
23 |
2.087 |
± |
1.505 |
|||
t: test value for T-test f: test value for ANOVA test
As shown in table (6) Demographic data & Awareness about Patient with history of CKD
Regarding Age: studes clarified that most of the The patients' age >50 ages with Mean± SD (2.714±1.586) while between age 35-40 year with Mean±SD (2.429 ±1.595) while 40-50 year with Mean± SD (2.308±1.797) follow by 30-35 years with Mean± SD (1.969±1.388) and age (25-29) year with Mean±SD (1.867±1.328) and a statistical significance (F= 2.249 p< 0.049)
Regarding six: studes clarified that most of the women patients were Mean± SD (1.963±1.330). while and men Mean± SD (2.159±1.562) with no statistically significance (T= -1.155, p 0.249)
Regarding Working years: In our research show that most of the participants>10 years with Mean± SD (2.652 ± 1.483) while 5-10 years with Mean± SD (2.038±1.330) follow by <5 years with Mean±SD (1.745±1.386) and statistically significance (F= 9.882 p 0.001)
Regarding Job title: In our research show that most of the participants the medical doctor with Mean±SD (2.194 ±1.657) while Nurse with Mean± SD (1.912 ± 1.192) and no statistically significance (T= 1.705 p 0.089)
Regarding Institute: Our research clarified that most of the participants in the King Faisal Medical Hospital Mean±SD (2.029±1.638) while in the Other Mean±SD (2.087±1.505) while in the King Abdul Aziz Specialist hospital with Mean±SD (2.029±1.638). Alhada Armed Forces Hospital with Mean±SD (1.937±1.223) and no statistical significance (F= 0.508 p< 0.677)
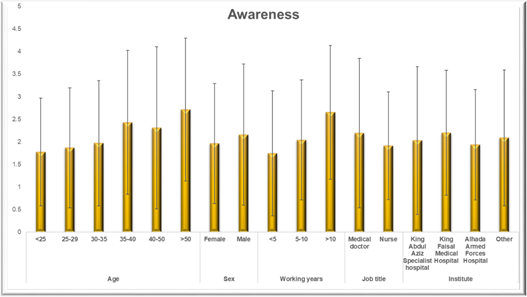
Figure (2): Histogram with normal curve Describe the relation of the demographic data (age, six, working years, job title, institute) and Awareness about Patient with a history of CKD
Discussion
The awareness of medical staff for vein saving in the patient with CKD The purpose of this is to help physicians and nurses to be better at preserving the patient's vein [1]. The study strongly reflects a focus on high-quality awareness of medical staff for vein saving the patients with chronic kidney disease (CKD) the objective of the study to determine the awareness of medical staff for vein saving in the patient with CKD in King Abdul-Aziz Specialist Hospital, King Faisal Hospital, and Armed Forces Hospital, Taif city, Saudi Arabia. The study included 315 medical staff in King Abdul-Aziz Specialist Hospital, King Faisal Hospital, and Armed Forces Hospital, Taif city, Saudi Arabia follow up and were enrolled in this study. Most of the participant were in the age range of (25-29) years were (38.1%), many of the patients' were female (60.0%), the majority of participant heave experience duration (5-10) had (33.3), the majority of participant were nurse (54.3) see table (1). Estimates of provider awareness of CKD Several studies indicate that only 22–30% of family practice physicians and general internists are aware of the existence of National Kidney Foundation (NKF) Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines, dealing with patients with CKD; in contrast, approximately 80% of the same physicians report that the American Diabetes Association (ADA) and Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC) guidelines influence CKD care [16]. The production of a successful arteriovenous fistula because of dialysis depends the central veins' existence healthy. Once the central vein is stenosis, creating a functioning arteriovenous fistula will be more difficult [15]. Awareness of CKD participants can be measured about other targeted groups for vein saving in the patient with CKD. The majority of participants answered no for the qustion “Do you know vein saving?” with the percentage of (50.2% ) followed by answer yes with the percentage of (49.8% )see table (3) . Health-care provider awareness of CKD can be measured in a variety of ways; accurate estimates the pervasivenessof provider awareness of CKD require an understanding of these degrees of awareness and different measures, including their strengths and limitations. [17] Current estimates on CKD Awareness indicate that each provider-level cognizance still unacceptably low. Awareness over CKD, among these together with CKD stage three and 4, also with albuminuria is lower than most appropriate yet has now not been improving over the last decade. [18]
According to the level of awareness, Patient with a history of CKD showed the weak awareness with the percentage of (47.0%) and high awareness with the percentage of (5.1%). Although, there is a significant relationship between the Score of the level of awareness, the p-value <0.001, Chi-square (X2 -125.19) ranging (0-6) and Mean± SD (2.041±1.428) see table (5).
The importance of CKD awareness at earlier stages of disease implementation of evidence-based medication regimens cannot be underestimated. Additional studies examining the effect of increased provider awareness on patient awareness of CKD and patient behavioral changes are key. Also, the effects of earlier CKD diagnosis the subsequent progression of kidney dysfunction and cardiovascular outcomes are essential to document and understand. Potential negative outcomes associated with increased provider awareness of CKD cannot be neglected. [19]. In our study, the majority of our participants were noticed that age >50 age with Mean± SD (2.714±1.586) while between age 35-40 year with Mean± SD (2.429 ±1.595) while a statistical significance of (F= 2.249 p< 0.049). Regarding Working years In our study, the majority of our participants were noticed >10 years with Mean± SD (2.652 ± 1.483) while 5-10 years with Mean± SD (2.038 ± 1.330) follow by <5 years with Mean± SD (1.745 ±1.386) and statistically significance (F= 9.882 p 0.001). see table (6). Vein preservation important to Patients with chronic kidney disease (CKD) may be on hemodialysis (HD) or may need HD in the future.
Conclusion
Must be improved levels of awareness among the doctors and nurses for vein saving in the patient with CKD in King Abdul-Aziz Specialist Hospital, King Faisal Hospital, and Armed Forces Hospital, Taif city, Saudi Arabia. More research is needed to manage the implementation of awareness campaigns. Additionally, further studies are essential to fully know the awareness the variables among thedoctors and nurses staff for vein saving in the patient with CKD However, because such studies will take time, efforts to increase awareness about vein saving in the patient Knowledge need to be implemented simultaneously with these studies, given the high prevalence of CKD and its risk factors.
References

