Pharmacophore an International Research Journal
COMPARISON OF OROPHARYNGEAL MANIFESTATIONS IN HOSPITALIZED PATIENTS WITH COVID-19 AND HIV/AIDS: A SINGLE CENTER RETROSPECTIVE STUDY
Adriana-Teodora Campeanu1, Cristian Delcea2*, Gheorghe-Mihail Banariu3, Aurora Craciun4, Sorina Ispas5, Laura Mariana Popa6, Mihaela Rus7, Radu Popa-Nedelcu8, Irina Magdalena Dumitru9
|
|
|
ABSTRACT
The COVID-19 pandemic has had a significant effect on people with HIV because of restricted access to treatment facilities. Oral health is crucial for preventing systemic problems, such as bacterial infections or septicemia. These are serious effects for immunocompromised individuals. Oral lesions are the initial clinical manifestations of HIV infection and act as dependable markers of immunosuppression. This highlights their crucial role in the early assessment, identification, and management of these individuals. This study examines the oral symptoms observed in 156 healthy, COVID-19, and HIV-infected individuals amid the COVID-19 pandemic.
The individuals recruited for this study were patients of the Constanța Clinical Hospital of Infectious Diseases, between April 2021 and October 2022 which delayed their visit to healthcare facilities because of restricted access during the pandemic. Two patients were COVID-19 positive, other 52 were diagnosed with HIV and receiving antiretroviral treatment, and 52 healthy individuals were recruited as the CONTROL group. The lesions were identified based on clinical examination and laboratory results. Oral lesions remain prevalent in HIV-infected individuals throughout the COVID-19 pandemic. They are significant clinical signs appearing early and affecting up to 74% of HIV-infected individuals (CD4+ T cells <1640uL). Oral health affects physical and emotional well-being by potentially compromising oral aesthetics and altering different functions of the mouth as well as reducing the quality of life for patients. It is essential to include oral in the medical care of HIV-positive patients.
Keywords: HIV patients, COVID-19 patients, Oral manifestations, Pandemic
Introduction
HIV, a disease, can lead to AIDS (acquired immunodeficiency syndrome) and remains an important medical concern [1]. HIV belongs to the lentivirus family and is a subtype of retroviruses. Maxillofacial symptoms are the primary and crucial sign of HIV infection [2].
Oral lesions can act as an early clinical sign of HIV infection and may indicate the progression of HIV to AIDS. They are utilized to assess the efficacy of anti-HIV treatment and are included in various stage protocols. Oral lesions can be an early sign of HIV infection and may indicate the progression of HIV to AIDS. They are utilized to assess the efficacy of anti-HIV treatment and are included in various stage protocols [3].
Oral symptoms in people with HIV are associated with a CD4+ lymphocyte count below 200 cells/mm3 and a high viral load, and can indicate HIV infection. As HIV infection advances, it is linked to specific oral issues such as Kaposi's sarcoma, hairy leukoplakia, and candidiasis. The extent of the lesion is determined based on the quantity of CD4+ cells [4].
Health practitioners must be able to recognise, diagnose, and treat oral diseases using clinical features, causes, and risk factors, both local and systemic [5].
Early identification of an injury enables the optimisation and prioritisation of dental therapy, particularly in acute conditions like gingivitis and necrotizing periodontitis.
In this patient population, it is crucial to prioritise the creation of strategies aimed at preventing, controlling, and reducing these diseases to decrease morbidity and death [6].
Oral lesions are seen in more than half of HIV-infected individuals and over 75% of AIDS patients. Antiretroviral treatment (ART) has led to a significant reduction in opportunistic infections, lower death rates, and improved survival and quality of life for those living with HIV [7].
Oral symptoms such as Kaposi’s sarcoma, oral candidiasis, and oral hairy leukoplakia are considered markers of the efficacy of ART. ART reduces saliva production and encourages an imbalance in the oral microbiota, leading to a change in the microbial community and making it easier for unusual bacteria to establish on-site [8]. The adverse effects of ART contribute to the development of oral problems such as xerostomia, leading to more severe and persistent oral diseases such as periodontal disease and dental caries [9]. Oral lesions linked to HIV/AIDS significantly affect the quality of life of patients since oral health is connected to both physical and mental well-being.
Some oral lesions are ulcerative and painful, leading to loss of taste, dental complications, compromised aesthetics, speech alterations, and difficulty in chewing and swallowing [9]. This can contribute to malnutrition and immune system dysfunction. Early and appropriate treatment of oral symptoms is necessary to decrease morbidity and death in this patient population [10].
Oral symptoms of HIV infection can be categorized as neoplasms, infections, immune-mediated problems, other disorders (such as nutritional concerns, parotid disease, and xerostomia), and oral signs resulting from the negative consequences of antiretroviral therapy [11].
Oral or pharyngeal candidiasis is the most common fungal infection observed as the initial indication of symptomatic HIV infection [12]. Oral hairy leukoplakia is associated with Epstein–Barr virus (EBV) infection.
Oral hairy leukoplakia and candidiasis are frequently linked to and categorized as AIDS-defining illnesses. According to the Centers for Disease Control and Prevention, they are also part of the clinical categorization of HIV [13]. In HIV patients, common infectious diseases include herpes simplex pneumonia, Salmonella infection, candidiasis, toxoplasmosis,
Cytomegalovirus-related ulcerations, oral warts from human papillomavirus, necrotizing ulcerative gingivitis, LGE, periodontitis, non-Hodgkin’s lymphoma, and Kaposi’s sarcoma are the most prevalent neoplasms among HIV patients [14]. Immune system problems may cause oral issues such as necrotizing stomatitis. xerostomia, and aphthous ulcers. Adverse effects of anti-retroviral medication may include cheilitis, oral hyperpigmentation, lip edema, paresthesia, erythema multiforme, xerostomia, and taste abnormalities [14].
COVID-19 is a respiratory transmissible disease that originated in China in December 2019. The World Health Organization categorized it as a pandemic in March 2020 [15]. The highly infectious nature of the COVID-19 pandemic instills fear in individuals, who tend to hold back from visiting healthcare institutions unless they are facing a life-threatening emergency [16].
During the COVID-19 pandemic, the number of COVID-19 cases has been fluctuating. People living with HIV have had substantial negative impacts on their access to healthcare services in the first phases of the COVID-19 pandemic, namely in relation to the limited availability of HIV testing and initiation of antiretroviral medication [17].
The patient's health remained unclear due to the delay in examining their state, which therefore led to a delay in administering HIV therapy. Many individuals are very susceptible to HIV infection because they have restricted access to preventative and curative services [18].
The use of antiretroviral therapy has resulted in a substantial decrease in the occurrence of opportunistic infections, decreased mortality rates, and enhanced longevity and well-being among those living with HIV.
Improvements in some oral disorders such as oral candidiasis or hairy leukoplakia and Kaposi’s sarcoma, are considered signs of the efficacy of antiretroviral treatment [19].
Dentists have a vital role in identifying oral lesions linked to HIV infection and AIDS via early detection screening. Oral symptoms are the first clinical indicators of HIV infection and deterioration of the immune system [20].
Oral lesions impact patients' well-being, influencing their mental and financial capabilities at both an individual and societal level. They might cause heightened morbidity due to the discomfort they produce [21].
Conditions such as herpes zoster affecting the trigeminal nerve or facial nerve palsy may lead to a deterioration in face appearance. Certain oral lesions, such as Kaposi's sarcoma, might lead to a deadly conclusion. Regular oral exams should be conducted in dental and medical settings for those with HIV and those who are at risk of the illness [22].
Materials and Methods
The cross-sectional research was performed on a cohort of 156 individuals who were visiting the Constanta Clinical Hospital for Infectious Diseases from April 2021 to October 2022. The research included two cohorts of patients: 52 HIV-infected individuals, 52 COVID-19-positive patients, and 52 patients in the CONTROL group who came for routine dentist check-ups.
All patients had examinations for oral lesions. Statistics and data analysis was performed using IBM SPSS version 26.
The information on the patients and their identities was anonymized. Participants received verbal and written explanations regarding the study's purpose, and written permission was collected.
Patients eligible for the study had to be diagnosed with either HIV or COVID-19 and be receiving antiretroviral medication regardless of age and sex. All eligible adult HIV/AIDS patients who visited the clinic were included in the study. Exclusion criteria included individuals who did not adhere to therapy and those who declined to participate in the trial.
A well-organized questionnaire was used to gather social and demographic information from the research participants, as well as information about any oropharyngeal manifestations during the pandemic.
The initial CD4 count and other information were gathered from medical records and relevant documentation. An extensive clinical examination of the mouth was performed using sterile gauze and spatula under artificial illumination. The periodontal status was evaluated by examining the presence of gingivitis and clinical mobility and then classified as either a periodontal disease with or without mobility.
Information on age, race, education, general and oral symptoms, and behavior was gathered for the three groups. The analysis of quantitative variables involved examining the minimum and maximum values, as well as computing the means, standard deviations, and medians. Qualitative variables were analyzed to establish absolute and relative frequencies, and group comparison was conducted using the t-test. The experiments were carried out at a significance level of 5%.
A total of 52 individuals who tested positive for HIV were screened and subsequently enrolled in the research. The CD4/CD8 ratio of each individual was obtained and all 52 individuals tested positive for HIV antibodies using the enzyme-linked immunosorbent assay (ELISA). The structured questionnaire was used to collect sociodemographic data.
The clinical history was extracted from the patient's medical records.
The statistical study was conducted using version 26 of the SPSS programme. The relationship between the subject variable and each kind of oral lesion was examined using a chi-square test.
Logistic regression analysis was employed to establish the relationship between oral symptoms and the CD4/CD8 ratio in the HIV group. The odds ratio and its corresponding 95% confidence interval were computed. The Mann-Whitney test was also performed. The PPV (positive predictive value) and NPV (negative predictive value) of certain oral symptoms were assessed for individuals with a low CD4+/CD8 ratio.
The positive predictive value refers to the likelihood that a patient has a CD4/CD8 ratio less than 0.30 when a certain oral symptom is present. The negative predictive value indicates the probability of the patient having a CD4/CD8 ratio higher than 0.30 in the absence of a specific oral symptom. The threshold for statistical significance was established at a p-value of 0.05 or less.
Results and Discussion
Since the beginning of the HIV/AIDS pandemic, the mouth has been essential in understanding the progression of the disease [23]. Oral signs are more likely to occur due to a decline in immunological function. Only a limited number of research have examined the correlation between the CD4/CD8 ratio and oral symptoms [24]. Oral candidiasis (OC) has been linked to an elevated number of CD8 lymphocytes and a decreased CD4/CD8 ratio [25].
Research conducted in Western nations has also shown a correlation between oral symptoms and a higher HIV viral load [26-29].
The current study examined a group of 52 HIV patients, another group of 52 COVID-19-positive patients, and a CONTROL group of another 52 healthy individuals to determine if there is a connection between oral manifestations and the ratio of CD4/CD8 counts and HIV viral load.
The study aims to evaluate the use of certain oral symptoms in diagnosing low CD4/CD8 ratios (<0.30) by determining the negative predictive value (NPV) and positive predictive value (PPV).
The demographic distribution of the 52 patients in the CONTROL group, with an age range of 24 to 68 years and a mean age of 32 years, included 40 men and 12 females.
Table 1. Oropharyngeal manifestations during the COVID-19 pandemic
|
Pathogens and symptoms |
COVID-19 group |
Control group |
HIV+ |
|||
|
n=156 |
n=52 |
% |
n=52 |
% |
n=52 |
% |
|
Candida |
19 |
36.5 |
14 |
26.9 |
37 |
71.1 |
|
Herpes |
21 |
40.4 |
16 |
30.8 |
34 |
65.3 |
|
Thrush |
24 |
46.2 |
20 |
38.5 |
29 |
55.7 |
|
Glossitis |
1 |
1.9 |
7 |
13.5 |
17 |
32.6 |
|
Tonsillitis |
16 |
30.8 |
31 |
59.6 |
22 |
42.3 |
|
Pharyngitis |
23 |
44.2 |
33 |
63.5 |
29 |
55.7 |
|
Oral cavity pain |
39 |
75.0 |
36 |
69.2 |
42 |
80.7 |
|
Bleeding |
18 |
34.6 |
39 |
57.7 |
28 |
53.8 |
|
Periodontal pockets |
6 |
11.5 |
13 |
25.0 |
17 |
32.6 |
|
Abscess |
8 |
15.4 |
14 |
26.9 |
16 |
30.7 |
|
Facial and oral lesions |
12 |
23.1 |
7 |
13.5 |
22 |
42.3 |
|
Teeth color changes |
16 |
69.2 |
28 |
53.8 |
18 |
34.6 |
|
Recurrence |
7 |
13.5 |
6 |
11.5 |
39 |
69.2 |
The group of patients with COVID-19 (n = 52) was investigated, and a certain percentage (mean = 16.15) of them had oral signs. Seventy-five of individuals in the COVID-19 group reported experiencing oral discomfort, and 69% showed changes in the color of teeth or tooth decay. A notable portion of patients had tonsillitis (30.2%), Candida (36.5%), thrush (46.2%), Herpes (40.4%), hemorrhage (34.6%) pharyngitis (44.2%). On the other hand, glossitis was encountered by just 1.9% of patients, with a minority reporting periodontal pockets (11.5%), abscesses (15.4%), various face and oral problems (23.1%), and recurrence (13.5%).
In the CONTROL group, the occurrence of oropharyngeal symptoms was less frequent than in the COVID-19 group, with the exception of pharyngitis (63.5%), tonsillitis (59.6%), glossitis (13.5%), abscesses (26.9%). hemorrhage (57.7%), periodontal pockets (25%), and
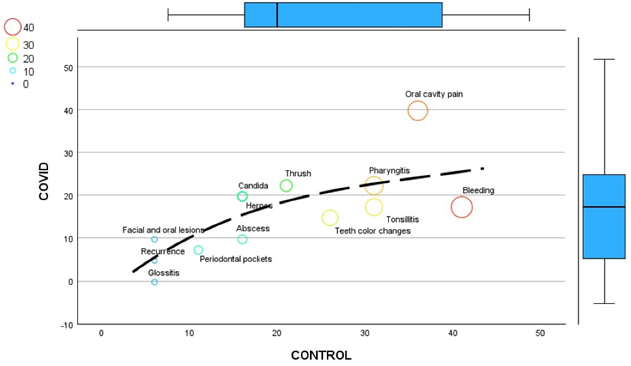
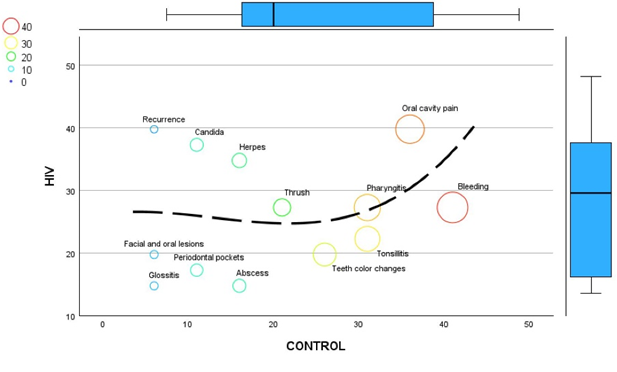
Figures 1 and 2 below show a regression variable plot with a regression line, demonstrating the position of HIV+ patients in relation to CONTROL and COVID-19 groups (Figure 1), and the position of COVID-19 patients in relationship with the CONTROL and HIV+ groups (Figure 2). It's particularly useful for visualizing how one variable (HIV in Figure 1, COVID-19 in Figure 2) affects another variable.
|
|
|
Figure 1. Trends in oropharyngeal manifestations of the HIV+ group when compared to the CONTROL and COVID-19 groups |
|
|
|
Figure 2. Trends in oropharyngeal manifestations of the COVID-19 group when compared to the CONTROL and HIV+ groups |
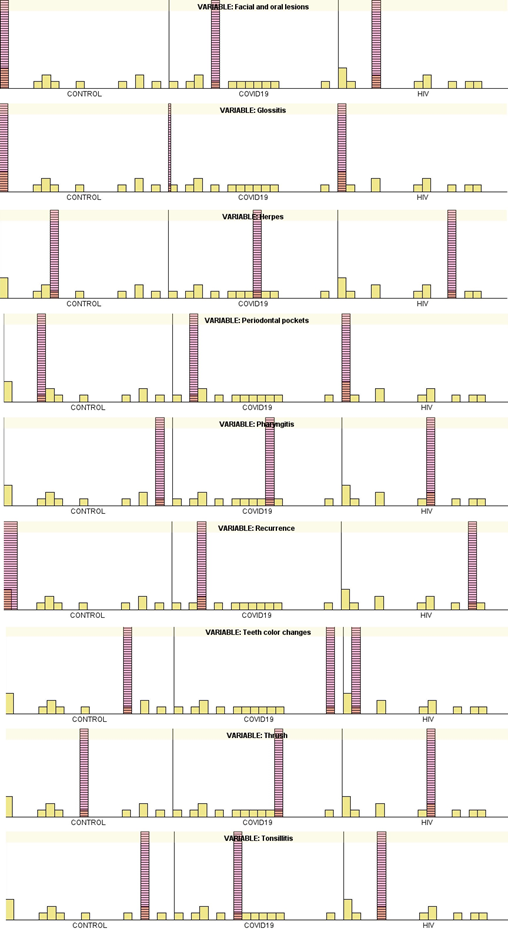
Figure 3 shows a comparison of oropharyngeal manifestations between the 3 groups. It can be seen that in various instances the HIV group has a higher percentage of patients. By looking at the position of the HIV+ lined column (coloured in pink), the further the column is from the x axis, the more prevalent that oropharyngeal manifestation is.
Thus, apart from “glossitis”, “periodontal pockets” and “teeth colour changes”, in all instances HIV+ group had the highest incidence of signs and symptoms.
|
|
|
Figure 3. Descriptive statistics to assess differences between oropharyngeal manifestations of CONTROL, COVID-19, and HIV+ patients (A) |
Both HIV and COVID-19 present with similar oropharyngeal symptoms such as sore throat, cough, and oral lesions. Comparing these manifestations can help clinicians differentiate between the two conditions, leading to accurate diagnosis and appropriate management
Comparing oropharyngeal manifestations can provide insights into the epidemiology and spread of HIV and COVID-19. Differences in symptomatology may impact public health measures such as screening, testing, contact tracing, and surveillance efforts.
Table 2 shows that the average absolute CD4 lymphocyte count for patients with a low CD4/CD8 ratio was 163.43 cells/mm3 (standard deviation 143.59). Patients in the second category had an average count of 325.00 cells/mm3 with a standard deviation of 167.46, whereas patients in the third subgroup had an average count of 502.33 cells/mm3 with a standard deviation of 290. When analyzing CD4 lymphocyte numbers to CD4/CD8 ratio in different groups, patients with low ratios showed significant differences compared to patients with higher ratios (P<.001).
Table 2. Demographic and clinical characteristics of HIV patients receiving antiretroviral therapy according to the CD4 cell count
|
Characteristic |
HIV Infection |
p Value |
||
|
CD3 700-2800 uL N=9 (18%) |
CD4 330-1640 uL N=14 (27%) |
CD8 2000->350 uL N=29 (55%) |
||
|
Sex, n (%) |
|
|
|
<0.05 |
|
Male |
4 (8%) |
7 (14%) |
15 (28%) |
<0.05 |
|
Female |
5 (9%) |
7 (14%) |
14 (27%) |
<0.05 |
|
Age, median years |
30 (33, 48) |
29 (28, 47) |
31 (25, 40) |
<0.05 |
|
CD4/CD8, median |
0.1 (0.1, 0.2) |
0.3 (0.2, 0.5) |
0.5 (0.4, 0.6) |
<0.05 |
Oral symptoms were also grouped based on different CD4/CD8 ratios. In group 1, loss of spicy taste was seen in 49.3% of cases, followed by sour taste in 40.6% and xerostomia in 37.7%. In group 2, loss of salty taste was the most prevalent oral symptom, observed in 28.6% of cases, followed by loss of spicy taste in 17.9%. The most prevalent observation was the loss of spicy taste (38.8%), followed by the loss of salty taste (35.9%), sour taste (32.0%), and sweet taste (17.5%).
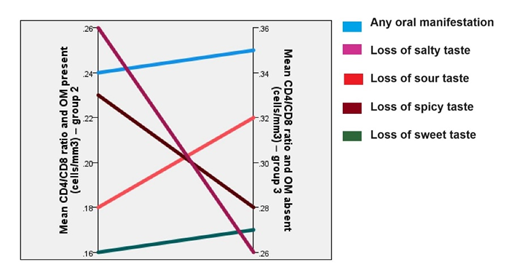
Table 3 shows the CD4/CD8 ratios for groups with and without oral symptoms. The average absolute CD4 count for those with any oral manifestation was 196.18 cells/mm3, and the average CD4/CD8 ratio was 0.24, with a standard variation of 0.22. People who had a decrease of sour taste had an average CD4/CD8 ratio of 0.16 and a mean absolute CD4 count of 126.78 cells/mm3.
The Mann-Whitney U test indicated a statistically significant difference in average values between the group exhibiting oral manifestations and the group lacking oral symptoms (P < 0.05). Significant statistical differences were seen for loss of spicy and sour taste among individual oral symptoms (P < 0.05).
The PPV and NPV were determined for the correlation with certain oral symptoms when compared with the CD4/CD8 ratio within the group. The positive predictive values for loss of spicy, salty, sour, and sweet taste were 85%, 77.8%, 77.8%, and 75.7%, respectively. The net present values for loss of taste were 44.4%, 34.3%, 35.3%, and 37.9%, respectively. A multivariate regression analysis was conducted to determine the odds ratio and a confidence interval of 95% for all oral symptoms associated with low CD4/CD8 ratios (<0.30). The odds ratio for low CD4/CD8 ratio in individuals with loss of spicy taste was 4.530, indicating a strong likelihood. No statistically significant findings were seen for any oral symptoms, as shown in Table 3.
Table 3. Mean CD4/CD8 ratio and their association with the presence or absence of oral manifestations
|
Oral manifestations (OM) |
Absolute mean CD4 count and OM present (cells/mm3)-group 1 |
Mean CD4/CD8 ratio and OM present (cells/mm3)-group 2 |
Mean CD4/CD8 ratio and OM absent (cells/mm3)-group 3 |
p Value |
|
Any oral manifestation |
196.18 |
0.24 (S.D-0.23) |
0.35 (S.D-0.17) |
0.01 |
|
Loss of spicy taste |
147.18 |
0.18 (S.D-0.12) |
0.32 (S.D-0.26) |
0.00 |
|
Loss of salty taste |
126.78 |
0.16 (S.D-0.15) |
0.27 (S.D-0.23) |
0.05 |
|
Loss of sour taste |
149.39 |
0.26 (S.D-0.23) |
0.26 (S.D-0.22) |
0.93 |
|
Loss of sweet taste |
192.27 |
0.23 (S.D-0.26) |
0.28 (S.D-0.20) |
0.08 |
Oral symptoms were also grouped based on different CD4/CD8 ratios.
Figure 4 shows the oropharyngeal manifestations according to the means of the CD8 and CD8 counts.
|
|
|
Figure 4. Mean CD4/CD8 ratio and their association with the presence or absence of oral manifestations |
A comprehensive knowledge of the immunopathogenesis of HIV infection is essential for the rational enhancement of treatment approaches and the advancement of immunotherapeutics and preventive vaccinations. Improved understanding of the oral manifestations of HIV/AIDS in both adults and children is important for dental healthcare providers globally.
It is crucial to acknowledge the extreme difficulty in identifying whether patients now have or are at risk of having HIV infection. This understanding should be included in the ongoing maintenance and revision of infection control strategies in clinical settings. Therefore, it is essential to include ongoing and meticulous dental care as an integral component of the therapy for individuals with HIV/AIDS. Dental health practitioners should prioritize preventing, diagnosing, treating, and managing oral symptoms [30]. Additionally, these professionals should be knowledgeable of the connection between immunological indicators and the development of oral lesions [31]. To address the HIV/AIDS epidemic, key components include supporting the World Universal Public Health System, ensuring widespread access to highly active antiretroviral therapy, and implementing harm reduction initiatives with political and financial backing from local governments [32].
In the field of general dentistry, a significant number of patients report experiencing xerostomia, which is often caused by the use of certain medications, mainly antidepressants and anxiolytics [33]. Xerostomia can potentially be a sign of Sjogren's syndrome. If a patient has HIV, xerostomia is likely caused by HIV salivary gland disease or is a side effect of antiretroviral treatment (ART) [34].
Patients with xerostomia, regardless of their HIV serostatus, should get proper guidance on the heightened susceptibility to dental caries, especially in the cervical and root areas, as well as gingival inflammation. Furthermore, the use of salivary substitutes and sialogogues may alleviate the symptoms of xerostomia [35]. Our investigation did not reveal significant socio-economic differences among the co-infected patients. These efforts should include both medical therapies and socio-economic policies that target the reduction of the impact of these illnesses on the most susceptible groups. It is essential to recognise that our results are mostly derived from an epidemiological assessment and do not take into account some significant viro-immunological aspects owing to the absence of particular patient data.
Dental Care of HIV+ Patients
Oral symptoms of HIV infection in adults are similar to those in adults, with differences in dental deterioration and perhaps the time of tooth eruption [36]. Adults with HIV infection may have a higher susceptibility to dental caries, which may harm permanent teeth, compared to healthy individuals.
Nevertheless, dental decay in adults infected with HIV seems to be mostly equivalent to that in other adults with chronic illnesses who are of similar age [37].
Salivary gland problems caused by inflammation or infection are the second most prevalent category of illnesses in individuals with HIV, with neoplastic lesions being the most frequent [38]. HIV-infected people are at significant risk of developing salivary non-Hodgkin lymphoma and other secondary malignant tumours, such as Kaposi's sarcoma. These tumours make up 10% of all malignant tumours in the salivary glands in individuals with HIV [39].
Dry mouth, known as xerostomia, is a frequently seen symptom in patients with HIV infection, and it may be attributed to several underlying factors. For instance, it may be seen with an increase in the size of the salivary glands in DILS [40]. Additionally, it has been shown to occur specifically with HAART, especially certain NRTIs and PIs. Antiretroviral drugs, including lamivudine, didanosine, and protease inhibitors, might lead to decreased production of saliva [41]. Furthermore, the prolonged use of non-HIV-related drugs, including several types of antidepressants, may also result in mouth dryness.
Several investigations have shown that anti-retroviral medication may have a therapeutic impact on the severity of COVID-19 infection [42-45]. This finding might potentially be another contributing element that influences the observed outcome.
Similarly, research conducted by researchers in 2021 revealed that patients with greater CD4 levels had increased rates of intubation [46]. This indicates that a stronger immune response in individuals with HIV may potentially be harmful compared to those who have a weaker immune system, especially when combined with the excessive activation of the immune system seen in COVID-19 [47].
It is crucial to acknowledge that these predictors often serve as markers of severe COVID-19 illness. HIV significantly elevates the likelihood of organ failure due to factors such as immunological dysregulation, chronic inflammation, and the administration of hepatotoxic drugs [48]. COVID-19, especially in its extreme manifestation, may lead to the widespread failure of numerous organs due to the virus directly invading the host's viral tissue and a cytokine storm that results in persistent inflammation [49]. Identifying individuals with HIV who are susceptible to organ dysfunction caused by drug toxicity, immune dysregulation, or chronic inflammatory conditions can assist healthcare providers in identifying specific groups of patients who may be at a greater risk of experiencing multiple organ dysfunction [38]. This can lead to early recognition and more personalised management of severe COVID-19 symptoms in this population, potentially reducing the risk of mortality [20].
Our study expands the existing research by providing a comprehensive representative examination of clinical outcomes in COVID-19 and HIV-positive individuals [32]. Despite the inherent constraints, our research has effectively provided a foundation for future in-depth studies to understand the intricacies of treating patients who are diagnosed with HIV and COVID-19 [49]. The findings of this research have the potential to greatly influence clinical practice and affect public health strategies.
Although our study provides valuable insights into the health consequences of individuals with both HIV and COVID-19 infections, it is important to acknowledge that there are several limitations to our research. First and foremost, possible coding errors, insufficient precise data, and the inability to monitor patient data longitudinally [50].
Furthermore, our research methodology permits the examination of correlation between variables, but it does not establish a cause-and-effect relationship. Despite our diligent attempts to reduce the influence of other factors using propensity score matching, there is a potential for persistent confounding variables.
Also, the reliability of HIV and COVID-19 diagnoses only relying on ICD codes may be subject to scrutiny. Also, our research did not take into account the level of compliance with HIV medication or the extent of immunosuppression, both of which might have a substantial impact on the outcomes of patients. Although we faced limitations, our study provides vital insights into the relationship between HIV and COVID-19, which is an area of growing interest.
Conclusion
Individuals with COVID-19 commonly experience olfactory and gustatory deficits, which may suggest the initial phases of disease progression.
Symptoms were more prevalent in the group infected with SARS-CoV-2 compared to the control group.
The COVID-19 and HIV groups had lower rates of oropharyngeal symptoms compared to the CONTROL group, except for abscesses (7.7%), tooth color changes (36.5%), oral cavity pain (30.8%), bleeding (34.6%), tonsillitis (17.3%), and recurrence (15.4%). The severity of the condition did not correlate with the usage of corticosteroid medication or antiviral therapy.
These symptoms might serve as a first indication of the illness and, if considered, could result in an early diagnosis, hence reducing the spread of infection in dental clinics.
The lack of comprehensive data, including particular anti-retroviral medication regimens, delays our capacity to make conclusive statements about the clinical relationship between HIV and COVID-19. Considering these constraints, our results should be regarded as a comprehensive epidemiological study on the outcomes of persons who are infected with both HIV and COVID-19.
Our analysis indicates specific regions that need further investigation and highlights the need for future research to better understand the association between these two illnesses. This involves identifying certain subgroups of individuals who are HIV-positive and may be more susceptible to experiencing negative clinical outcomes as a result of COVID-19. This contributes to a more thorough understanding of the overlapping nature of these illnesses.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: None