Pharmacophore an International Research Journal
IDENTIFICATION AND DIAGNOSIS OF POSSIBLE MUTATIONS IN HUMAN P-53 LYMPHOCYTES
Nica-Badea Delia1, Tataru Tiberiu1, Marinas Marius Cristian2*, Băleanu Vlad1, Udriștioiu Aurelian3, Tataru Paula1, Tenea Cojan Tiberiu Stefanita4
|
|
|
ABSTRACT
This study looked at a few confirmed cases of chronic lymphocytic leukemia (CLL) that may have had mutations in the human B lymphocyte genome's P-53 gene. The ELISA technique was used to determine the frequency of p-53 protein expression in twenty CLL patients undergoing evaluation in stages II–III / IV. In 17 of the 20 cases, the average amounts of p-53 proteins were found to be 16.76 μg/dl, with a probability index of p = 0.034 and a CV of 0.5%. It was discovered that as the illness progressed, the proportion of p-53 positive isoform proteins rose above normal. The percentage was 15% ± 2 in stages 1-2 and 100% in stages 3-4. Recent studies have shown that the p-53 protein inhibits protein kinase B, the AMPK protein, and the mTOR complex, hence mediating genes that trigger autophagy and stimulating autophagy. One potential use of the p-53 protein's role in cancer cell autophagy is the development of a novel anti-cancer medicinal approach. When a patient develops resistance to the initial line of treatment, the ELISA approach has shown to be an invaluable prognostic tool for CLL, enabling the administration of customized medication.
Keywords: Type B chronic lymphocytic leukaemia, P-53 gene, Intrinsic apoptosis, CD-5 receptor, ELISA
Introduction
Chronic B lymphocytic leukemia (CLL-B) is the most prevalent kind of leukemia in adults and older people. Depending on the patient's age or gender, it might manifest in a variety of ways clinically. Phosphoproteins p-53 and p-21 are thought to be significantly significant among the variables that govern and control the apoptotic process and disease development in patients. There are now a number of paraclinical research techniques that can be used to forecast how the disease will proceed [1]. In recent years, it has been found that the carcinogenesis process is triggered by the synthesis of a certain percentage of mutant p-53 proteins in type B lymphocytes, which increase in stability. As a result of this finding, the p-53 protein was identified and measured using a variety of techniques, including sandwich enzyme-linked immunosorbent assay (sandwich ELISA), single-stranded peptide microarray (SSPMa), polymerase chain reaction (PCR), and next-generation sequencing (NGS) [2].
Certain chromosomal anomalies, such as variations in BCL-2, TCL1, and ZAP-70 gene expressions and micro-RNA forms, can function as prognostic and diagnostic markers for the course and prognosis of CCL-B illness. In this scientific setting, individuals with CLL-B who have these molecular abnormalities should be evaluated for potential treatment drugs [3].
Hereditary cancer susceptibility syndrome (Li Fraumeni) is caused by a single allele of the TP-53 gene, which is mutated often in human neoplasia. This variation may impair the transcriptional activity of the p-53 protein because it encodes different isoforms of the protein [4-7].
Materials and Methods
The frequency of p-53 protein expression in 20 typical CLL-B patients was investigated by the ELISA method in order to investigate the relationship between the p-53 protein at different stages of the disease and its impact on the longevity of patients [8]. ELISA Kit Part Number: Standard 96-well Coated Strip Plate 1 (Lyophilized) Assay and Diluent (5x) in 2 vials 1 vial x 15 ml, 2 vials of HRP-Streptavidin Conjugate (800x), Biotinylated Detection Antibody One 200 µl vial of Wash Buffer (20x) One 25 ml vial, one 12 ml vial of TMB substrate, and one vial of Stop Solution sulfuric acid (H2SO4) One 8 ml vial of Plate Sealers.
Under denaturing conditions, the monoclonal p-53 antibody PAb 240, which is employed in the ELISA technique, can distinguish between mutant and wild-type p-53. According to the prospect, species reactivity is for either rhesus monkeys or humans. In its wild-type conformation, the p-53 protein is structurally buried, but when the p-53 protein is denaturated or adopts a mutant conformation—where point mutations in the P-53 gene alter the p-53 protein's terminal structure—the monoclonal antibody PAb 240 identifies an epitope that has become revealed. It is advised to use this ELISA kit with serum, plasma, or tissue homogenates. It is not recommended to use other kinds of samples.
The following procedures were followed in order to separate lymphocytes from whole blood using a Ficoll:
The lymphocytes were extracted and resuspended in tampon phosphate (PBS) following three rounds of washing and ultrasonic cell lysis from the CLL patients' EDTA samples, which had been centrifuged and the supernatants removed. The residual cell debris was subsequently removed with four rounds of centrifugation at 1500 x g for 10 minutes at a temperature between 2 and 8 °C. There was also an option to freeze the cells at -20 °C and then thaw them for three hours at room temperature.
100 μl of the suitable antibody (capture antibody) was added to each microtiter plate well at a rate of 1–10 μg/mL in the coating buffer. Following a full night of covering and incubation at 4 °C, the plate was washed three times using ELISA Wash Buffer. Each well received 150 μL of blocking solution, and it was then incubated for 60 minutes at 37 °C. The combination was then cleaned four more times in a wash buffer. Following the sample dilution process with wash buffer (ELISA), 100 μL of the target antigen and appropriately diluted standards were added to the appropriate wells. Following a 90-minute incubation period at 37 °C, the combination underwent three careful washes in the wash buffer.
Next, each well received 100 μL of the conjugate detection antibody (Streptavidin HPR Complex), which was then incubated for an hour at 37 °C. The resultant mixture was then rinsed three times in wash buffer, and each well received 100 μL of a suitable substrate solution (TMB). This was then incubated at room temperature (and in darkness) for 30 minutes, or until the color of the well contents changed. Finally, an H2SO4 stop solution was added, and a series of dilutions of the positive control standard were carried out in duplicate or triplicate, with the final well serving as the negative control mark.
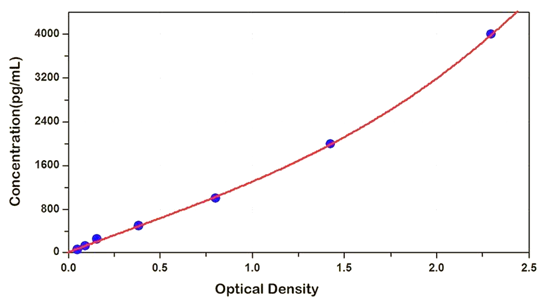
Plotting a standard curve with the linear absorbance data on the y-axis and the serial dilution data on the x-axis (logarithmic scale) allowed for identification. The published literature may provide information on the antigen concentrations in the various kinds of samples. Nonetheless, it is sometimes required to do a number of dilutions for any kind of material. The optical density (OD) value of 450 nm ± 2 nm on the ELISA line was proportionate to the quantity of p-53 protein, and a colored product forms in proportion to the concentration of human p53 protein present in the samples. The OD of the samples was compared to the standard curve in order to determine the concentration of p-53 protein in the samples. Additionally, duplicate or triplicate samples were measured [9] (Figure 1).
|
|
|
Figure 1. Standard curve from serial dilution data with the x-axis (logarithmic scale) vs. Y-axis (linear) absorption |
Every patient who arrived at the hospital exhibiting signs and symptoms, including coughs, sweats at night, and discomfort in the retrosternum, was put through a thorough medical examination. Adenopathy and/or splenomegaly were discovered by clinical examination and ultrasounds, with the spleen enlarging by 3 cm beyond its usual dimensions.
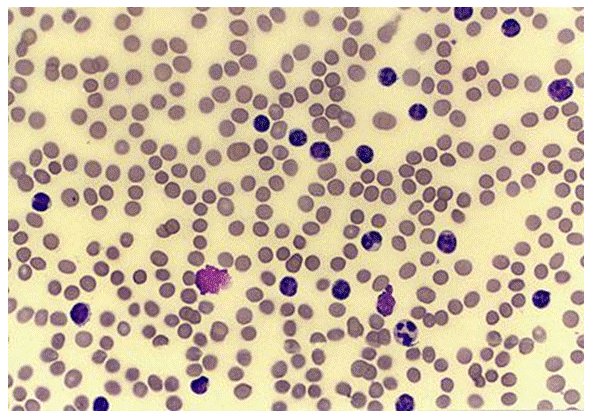
A hemogram was performed in each case using a 5-Diff Hematology Analyzer, and May-Grunwald-Giemsa staining was utilized for blood smear cytology studies on peripheral blood and medullary bone marrow. The leukemia cells in the peripheral blood smear were identified by their distinctive microscopic appearance. The tiny nuclei of the cells were adult lymphocytes without nucleoli and with complete or partially aggregated chromatin (Figure 2).
|
|
|
Figure 2. The appearance of microscopic smear in Chronic Lymphocytic Leukemia (CLL). Numerous small lymphocytes with an incised nucleus disposed of peripheral blood |
The laboratory hematological diagnosis of CLL type B was validated by immunophenotyping with monoclonal antibodies (flow cytometry) and B cells producing IgM or IgG heavy chains with kappa or lambda light chains. The CD5⁺, CD19⁺, CD20⁺, CD23⁺, and CD28⁺ receptors were examined using monoclonal antibodies. Patients with CLL-B (chronic lymphocytic leukemia) were identified, the disease's clinical stages were established, and the patients' reactions to therapy were evaluated based on guidelines provided by the International CLL Workshop [6]. The CCL illness patients under examination were chosen based on the presence of blood films on microscopic slides containing fewer than 10% prolymphocytes and the absolute quantity of lymphocytes (>5000) in the hemogram with differential count revealed within the preceding three months. For analysis, peripheral blood films were employed, and the May-Grunwald Giemsa hematological solution was utilized to stain them. Using the flow cytometry approach, cases with CD19⁺, CD20⁻, CD5⁺, and CD23⁺ were recruited for the research.
There were 22 patients in Stage B (patients with stable illness) who were considered ineligible for this trial after completing a full year of treatment with normal hemogram readings and responding to rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) first-line treatment. Following their diagnosis in the first year of CLL, eighteen (18) individuals in Stage A (0) (diagnosed patients without treatment) continued to be monitored by doctors. Binet provides the CCL stage categorization that is being discussed. Twenty patients who were classified as "failure to complete" or "partial remission" after a year of R-CHOP treatment resistance a term used to describe patients following the B/C Binet disease phase—were included in this research. At the time of this investigation, all 20 patients were receiving treatment, and more than 80% of their peripheral blood contained leukemic B cells. Blood samples for CLL-B [8] were taken from patients hospitalized between November 2015 and September 2019 at the Hospital University of Bucharest's Hematology Departments.
Results and Discussion
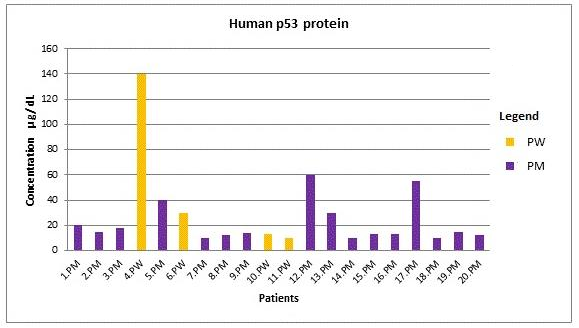
Six of the 20 patients in the study were women, ages 39 to 85, and 14 of the patients were men. Cytostatic and CLL-specific immunotherapy were being administered to patients at the time of this research. As shown in Figure 3, the findings of protein concentration p-53 detection for males were 20, 15, 18, 40, 10, 12, 14, 60, 30, 10, 13, 13, 5, 10, 15, 12, (µg/dl) and for women, the results were 140, 30, 13, 10, (µg/dl).
|
|
|
Figure 3. Values of p-53 protein co-concentration, assays performed on the ELISA line. |
The interpretations of the statistics are as follows: With a probability index (NORMDIST) p of 0.034, STDEV = 8.35, CV = 0.5%, and an average p-53 protein concentration of 16.76 µg/dl were found in the 17 instances with p-53 protein expression (not including the three out-of-line cases included in the research). A reference interval of 24.5 µg/dl was established, with values ranging from 10 to 40 µg/dl.
The concentration of the p-53 protein mutant was determined to be 60 µg/dl in two males and 140 µg/dl in one woman, based on data gathered from specialist literature, representing the pathogenic values in the three instances with greatly increased p-53. Men are more likely than women to have chronic lymphocytic leukemia, with a ratio of 2:1. Out of the 20 instances that were examined, 3 cases had a p53 protein positive rate of 15% overall in the increasing number of CLL cases. A significantly reduced response to treatment (p = 0.034) was linked to the presence of high-concentration p53 proteins in stage 2/3 of the illness (Table 1).
Table 1. Expression of hemogram parameters and p53 protein concentration in different stages of CLL-B
|
CLL Stage |
No. patients |
P-53 protein * Average values |
P53 isoform proteins Elevated values |
Hematological parameters** |
P value |
|
I/II |
17 |
16.76 μg / dL |
- |
Leukocyte = 35-50 x 10 3 / dL Hb = 11.8g / dL Platelets = 140 x 10 3 /dL Lymphocytes = 65-80% |
0.034 |
|
III/IV |
3 |
- |
15% |
Leucocytes = 250-500 x 10 3 /dL Hb = 8.6g / dL platelets = 45x10 3 / dL Lymphocytes = 85-90% |
0.05 |
*concentration in reactive lymphocytes B
**in peripheral blood
The following was used for statistical interpretation: method sensitivity (MS) = number of cases with abnormal values of tumor marker (p-53 > 10 μg/dL) / total number of cases positive for p-53 protein x 100 = 15/20 = 75%, indicating good sensitivity (normal value = 60-90%, CI 9%).Specificity of the method (SP) = number of cases with normal p-53 protein level (range 10–40) / total number of CLL-B patients (20) x 100 = 17/20 = 85%, which is good specificity (normal). Value = (70 to 90%, CI 95%); Positive predictive value (PPV) of this method = number of cases with true outliers of p-53 (p-53 variants = 3) / number of cases with p-53 true outliers’ Total number of cases with abnormal values (including p-53 variants) above the cutoff x 100 = 3/3 = 100% (CI 95%).
Using the calculation for the "t" statistic, it was found that "t" = 2. 2.01 and − 2.01 are the critical values derived from the "t" distribution over 20 degrees of freedom for a two-sided test at the conventional significance level of α = 0.05. It is not possible to reject the null hypothesis with a 95% confidence level since the computed "t" does not surpass these values. You may compute the student’s t-test using the Eq. 1 above, where "x" represents the sample mean, "s" the sample standard deviation, and "n" the sample size (Table 1).
|
t = (mean - µ) ⁄ (s/√n) |
(1) |
For this formula, t = 2.01 in the equation feature. In this test, n − 1 was the degree of freedom. Therefore, even though the patient population did not have to be normal, the distribution of the sample means was assumed to be.
Numerous studies have shown that TP-53 gene mutations are commonly detected in two chromosome 17p alleles and constitute over 15% of CLL patients. Compared to individuals who only have one of the 17p alleles deleted, patients with similar anomalies in both alleles exhibit greater resistance to therapy [10, 11].
In the experiment reported, with n = 17 patients, the average p-53 protein concentration in CLL was determined to be 16.76 µg/dl. According to Table 1, the average hemogram results are as follows: leukocyte numberer = 35–50 x 103/dL, platelets = 140 x 103/dL, hemoglobin = 11.8 g/dL, and lymphocytes in peripheral blood = 65–80%.
Statistics: The average p-53 protein concentration was found to be 16.76 µg/dL in the 17 instances with p-53 protein expression after the three out-of-line cases were excluded from the study. Table 1 shows that in the CLL stage III/IV (n = 3 patients), p53 isoform protein proportion with elevated values was present in 15% (3 of 20 cases); 2 men had values of 50μg and 60μg/dL, respectively, and 1 female had a value of 140μg/dL (p-value 0.034); hematological parameters in peripheral blood were altered, with leukocyte numbers of 250–500 x 10 3 /dL, Hb = 8.6g/dl, thrombocytosis = 45x10 3 /dL, and lymphocytes in peripheral blood = 85–90% (p-value =).
In several global investigations, immunohistochemistry (IHC) was used to assess the immune traits of CLL patients who tested positive for the p-53 protein. 47 patients participated in the study's second component, which looked at CLL in stages I and II. In 16.7% of the samples (7 out of 42 instances) that were examined, the P-53 protein isoform concentration in reactive lymphocyte B was discovered. Peripheral blood was found to have the following hematological parameters: leucocyte number = 35x10³/dl, Hb = 12,2g/d, thrombocyte = 140x10³/dL, and lymphocytes = 75–80%. The fraction of p53 isoform varied from 7 to 32%, and the average p-53 protein concentration in CLL in stage III/IV (n = 140 patients) was 47 U/m. Table 1 shows that the hematological parameters in peripheral blood were altered to include leukocytes (350 x 10³ / dL), hemoglobin (10,8 g / dL), thrombocytes (80 x 10³ / dL), and lymphocytes (80–90%). The percentage of peripheral blood that tested positive for p-53 was 15%.
According to recent research, the TP-53 gene is a tumor suppressor, meaning that when it is active, cancer cannot grow. When the nuclear protein p-53 attaches to DNA in a tumor cell, it activates the gene CDKN1A, which results in the production of the protein p-21. This protein then interacts with CDKN2 to prevent cell proliferation when DNA damage occurs. It is known that the nuclear p-53 protein protects the cell from malignant processes, whereas the cytoplasmic p-53 protein, through its isoforms, may acquire new capabilities to promote carcinogenesis processes [12-14]. The changed activity of the p-53 protein isoform affects the phenotype of tumor cells as well as DNA damage. Based on these findings, it appears that phosphorylating the p-53 protein with the amino acid serine-15 is a major target for p-53 activation. The partial inability of p-53 to block the advancement of the cell cycle is caused by the substitution of the amino acid alanine for serine. Furthermore, it has been shown that both the GLUT1 and GLUT4 receptors' transcriptional suppression occurs, and the p-53 protein is a significant regulator of glucose transport. In contrast, the malignant cell's GLUT1 and GLUT4 receptor activity is unaffected by the p-53 mutation.
The intracellular ATP concentrations (i-ATP) in malignant tissues were shown to be 10 times higher in the range of 200 to over 500 3M in vitro compared to normal tissues in the earlier study13. Internalized "I"-ATP accelerates cell growth, boosts cell survival, and keeps the cell in an anti-apoptotic state via binding the p-53 isoform proteins through phosphor-ester linkages. In more recent research, it was demonstrated that ATP analogue blocking significantly decreased cancer patients' resistance to targeted treatment [15-17].
High production of the MDM2 protein is one way that might cause TP-53 malfunction, according to another study [10, 11]. Since the micro-ARN, miR-34a, is involved in the induction of apoptosis and cell cycle disruption, its overexpression and its effect on increasing the intensity of CD20, FMC7, and CD79b receptors on the B cell surface may lead to increasingly aggressive It is related to the course of events of disease [18]. Additionally, miRNA genes such as the TP-53 gene and miR-34a, a downstream effector of p-53, are repressed by this protein [19].
Furthermore, ZAP-70 protein kinase, unmutated IGHV chains, and increased expression of CD38 receptors [18, 20] have all been connected to the 17p chromosomal deletion's poor prognosis for this subset of ZAP70 patients with CLL [20, 21]. Moreover, it was shown that a number of anti-malignant drugs might more effectively target tumors with autophagic abnormalities [22-24].
The p-53 protein inhibits the AMPK protein, the mTOR complex, and protein kinase B, which in turn mediates genes that promote and induce autophagy, according to several studies completed in the last few years [25, 26]. A novel anti-cancer therapy strategy may be developed by using the function of the p-53 protein in the autophagy of cancer cells [27].
Conclusion
The Elisa technique can be used as a screening tool to track the progression of stages of type B chronic lymphocytic leukemia that do not meet the usual criteria for treating malignant hematological diseases because of deletions or mutations of the P-53 gene that result in non-functional p-53 proteins [28].
Based on the presence of p-53 isoform protein and TP-53 gene mutations, this straightforward and reasonably priced ELISA method, like the one used in this study, is helpful in identifying patients who should be given consideration for personalized therapeutic strategies in the context of a heterogeneous malignant disease like CLL-B.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: None