Pharmacophore an International Research Journal
Pregnancy-Associated Gastric Cancer: Real-Life Diagnosis and Management
Onisâi Minodora1*, Vlădăreanu Ana-Maria1, Iordan Iuliana2, Bumbea Horia1 ,Nica Adriana3, Aliuș Cătălin4, Grădinaru Sebastian5, Roxana Bohiltea6, Monica Carstoiu6
|
|
|
Abstract
Pregnancy-associated gastric cancer is rare and has a poor prognosis. Most cases present at an advanced stage, the diagnosis often being delayed because the symptoms may mimic those of normal pregnancies. Also, treatment options are limited: surgical resection is an option for about half of the patients, chemotherapy regimens may have serious consequences for the fetus – often termination of pregnancy may be required, and the prognosis is dismal. We report the case of a 39-year-old female, 23 weeks pregnant, who presented with nausea, vomiting, and significant weight loss. Laboratory tests showed hypochromic microcytic anemia, thrombocytopenia, left shift with leukoerythroblastosis. Bone marrow aspiration was suggestive for metastases. Further investigations established the diagnosis of poorly differentiated gastric adenocarcinoma stage IV.
Keywords: gastric cancer, pregnancy, bone marrow metastases.
essentially a physiological event that causes many physical, psychological and social changes in women [2-4].
Malignancy is a rare event in pregnancy, complicating approximately 1:1000 pregnancies annually. [5] Diagnosis is often missed or delayed, as symptoms are usually attributed to pregnancy and most imaging studies [computed tomography (CT), positron emission tomography (PET)] are unsafe for the fetus. Furthermore, management is complicated by risks for both mother and baby. The most “common” pregnancy-associated cancers are cervical cancer, breast cancer, melanoma, lymphoma, and leukemia. [6]
Case History:
A 39-year-old female, gravida-three, para-two, 23-weeks pregnant, presented for nausea, vomiting, and weight loss (12kg since pregnant). Her medical history was significant for iron deficiency anemia treated with iron supplements. Laboratory tests showed hypochromic microcytic anemia [hemoglobin (HGB)=7g/dl], thrombocytopenia [platelet count (PLT)=70000/mmc], left shift with leukoerythroblastosis, normal hepatic and renal tests, normal coagulogram, elevated creatine kinase (CK=285U/L) and CKMB (515U/L).
She then developed rapidly progressive anemia (HGB=5.5g/dl) and thrombocytopenia (PLT=20000/mmc), hypofibrinogenemia (122mg/dl), elevated lactate dehydrogenase (LDH=700U/L).
A bone marrow aspiration was performed, revealing hypercellularity, numerous groups of large cells, with abundant, basophilic, vacuolated, and foamy cytoplasm, and round nuclei, suggestive for metastases of unclear origin (Figure1).
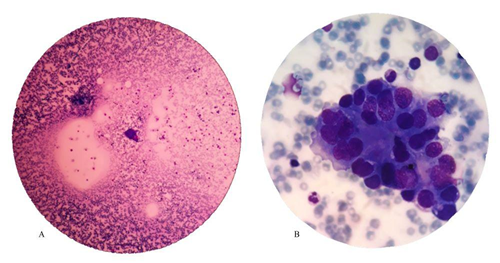
Figure 1: Microscopic images – marrow involvement with non-hematopoietic tumor cells (marrow metastases) - May–Grünwald–Giemsa stain 40x(A), respectively 100x(B)
Tumor markers were positive for alpha-fetoprotein, carcinoembryonic antigen, CA125, and CA19-9, the latter being particularly high (>2044U/ml).
Abdominal ultrasonography showed images suggestive for hepatic metastases, peripancreatic adenopathies, and splenomegaly. The esophagogastroduodenoscopy detected gastric stasis (food content mixed with blood) and a mass in the stomach body, exhibiting infiltrative characteristics, and occupying two-thirds of the gastric circumference (Figure2) – biopsies were taken.
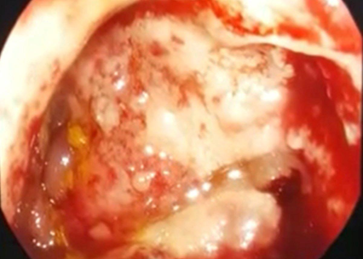
Figure 2: Endoscopic view of the gastric infiltrative tumor
At about 48 hours from admission, she developed dyspnea, polypnea, and hypoxemia. Suspecting pulmonary embolism, electrocardiogram, and cardiac ultrasonography were performed, but neither confirmed the diagnosis. An emergency CT was performed, which revealed ground-glass opacities and pulmonary nodules in both lungs, circumferential thickening of the gastric wall (23mm maximum), hepatosplenomegaly, and multiple abdominal and thoracic adenopathies.
Histopathological examination eventually confirmed poorly differentiated adenocarcinoma of the gastric antrum. The final diagnosis was stage IV (T2N3M1) gastric cancer, poorly differentiated adenocarcinoma, with multiple metastases.
Given the advanced status of the disease, with multiple metastases, severe respiratory and hematological degradation, lack of response to transfusion support, and rapid progression of the disease, the oncology, and surgical specialists decided that the patient was not eligible to receive radical surgical treatment (gastrectomy), radiotherapy, or chemotherapy, but only palliative care.
The evolution was extremely aggressive, with respiratory degradation and severe thrombocytopenia, aggravated by disseminated intravascular coagulation and medullary infiltration. The patient needed tracheal intubation and mechanical ventilation in less than four days since admission, with subsequent cardiac arrest.
Discussion:
Gastric cancer is a leading cause of cancer-related mortality worldwide, although due to screening programs, its incidence has decreased over the last few years. It is generally diagnosed in the elderly, but approximately 10% of cases appear in patients under 45 years old. [7] Pregnancy-associated gastric cancer is very rare - 0.025%-0.1% [8] of all pregnancies. Difficulties are related to the presentation at an advanced stage; longer time from diagnosis to treatment (median period of 21days); surgical resection is possible in 45-56% of cases; [9] chemotherapy is difficult to apply. All these lead to a dismal prognosis, with a median survival rate of 7months. [10]
Pregnancy causes changes in the gastrointestinal tract, which generate nausea, emesis, and gastroesophageal reflux. Acute abdomen symptoms during pregnancy pose a challenge in clinical diagnosis, radiological evaluation, and treatment. Heightened physician awareness on possible etiologies such as appendicitis [11], diverticulitis, incarcerated diaphragmatic hernia [12] and rarely digestive tract cancer, is required for rapid diagnosis and treatment to improve maternal/fetal outcome.
At admission, the blood count showed hypochromic anemia, thrombocytopenia, and left shift with leukoerythroblastosis. We excluded pure iron deficiency anemia because it was not explaining the progressive thrombocytopenia. Many cases of thrombocytopenia in pregnancy are physiologic, but about one-third are associated with potentially serious disorders, including preeclampsia, HELLP syndrome, sepsis, disseminated intravascular coagulation (DIC), thrombotic thrombocytopenic purpura (TTP), and malignant diseases. [13-16] We also considered TTP, but no schistocytes were seen on the peripheral blood smear, bilirubin, and creatinine levels were normal, and no renal or neurological anomalies or fever were observed. Anemia, thrombocytopenia, nausea, and vomiting also appear during HELLP syndrome, but there was no high blood pressure or proteinuria. Bone marrow aspiration unexpectedly raised the suspicion of metastatic malignancy as a cause for both laboratory and clinical anomalies, and further investigations established the origin.
Our patient was treated for severe and extended hyperemesis gravidum and pregnancy-related iron deficiency anemia, the most common and probable causes for her clinical status. Also, the patient herself delayed presenting to the hospital, as she considered the symptomatology to be “normal”. All these postponed the diagnosis.
Treatment options are limited. Here, radical oncologic surgery (gastrectomy) was not an option because of the advanced stage at diagnosis. Chemotherapy depends on gestational age and stage of the disease. Before 22 weeks, therapeutic abortion is recommended; after the second trimester, there are no major differences in the incidence of malformations between infants from normal pregnancies and those exposed to chemotherapy. There is no standard regimen for treatment during pregnancy. [17] Most patients only receive palliative chemotherapy due to the advanced stage at diagnosis.
Consequently, an emergency multidisciplinary approach is essential for proper diagnosis and treatment plan when dealing with any sort of pregnancy-associated malignancy.
We must consider that pregnancy is a physiological condition and that this kind of disorder is a very rare association. However, persistent severe symptoms, especially accompanied by signs of consumption (e.g. weight loss) should not be disregarded and should always point toward further investigation.
Conclusion:
The diagnosis of pregnancy-associated gastric cancer is frequently at an advanced stage because the symptoms are often written off as normal, and some imaging studies are prohibited. The treatment plan should take into consideration both the clinical stage and gestational age, but the diagnosis is often delayed, and the prognosis is usually very unfavorable.
The patient has signed the informed consent for the academic use of the medical data.
Acknowledgement:
We would like to thank our colleagues for their contribution to the case management and their every-day work and dedication: Cristina Ciufu, Anca Nicolescu, Mihaela Gaman, Daniela Vasile, Cristina Marinescu, Diana Cisleanu, Irina Voican, Andreea Spinu, Horia Pantu, El Khatib Ahed, Sorin Oprescu, Roxana Bohiltea, Monica Cirstoiu, Angelica Bratu, Oana Dumitrascu.
Key Messages: Guidelines are difficult to apply in real-life management of patients. We report pregnancy-associated cancer with fulminant evolution. Although such associations are rare, the prognosis is dismal, thus symptoms should not be disregarded, and prompt intervention is a must.
References

