Pharmacophore an International Research Journal
Moderated Moderation of Gender and Knowledge on The Relation Between Burden of Care and Quality of Life Among Caregivers of Schizophrenia
Areej Ghourmulla Alghamdi 1, Khushnoor Khan2*
|
|
|
Abstract
The current study focuses on the moderated moderation effect of gender and knowledge of caregivers about Schizophrenia on the relation between the Burden of Care (BOC) and Quality of Life (QOL). Data for the present study were collected from 150 caregivers of Schizophrenic patients using the snowball-sampling technique. Moderated moderation among the study variables was examined using a procedure developed by Dr.Andrew Hayes commonly known as ‘PROCESS’ which works with SPSS. The results of the study revealed that Knowledge significantly moderates the relation between BOC and QOL, but this moderation is moderated by the gender of the caregivers. For a visual representation of the moderation and moderated moderation effects, relevant graphs are produced. Results of the current study will provide guidelines for medical practitioners in devising such training programs, that shall simultaneously, reduce BOC and enhance QOL for caregivers of Schizophrenic patients keeping in view the gender of the caregivers. For the present study easy-to-follow approach is adopted with minimum cognitive jumps so that the procedure of the study can be replicated using other health care variables.
Keywords: Burden of Care, Quality of Life, Knowledge, Caregivers, Schizophrenia, Moderated-moderation.
Introduction
Right from the onset of the study let us see what schizophrenia is and how does it affect humans. Schizophrenia is in fact a sort of thinking and perception distortion, coupled with inept or blunted affect. Though certain cognitive deficits may evolve (ICD-10) clear consciousness and intellectual functioning remain intact. The main feature of schizophrenia has been abnormal behavior but the lessening of social functioning is a permanent feature of schizophrenia. Delusions and Hallucinations cannot be quoted as explicit symptoms of schizophrenic patients, but the salient evidence is a dysfunction of social behavior and even taking care of oneself [1]. has defined a caregiver as a family member living with the patient and has been meticulously associated in his/her activities covering all spectrum of life.
The burden of Care (BOC): [1] defined BOC as the presence of problems, difficulties, or adverse effects that affect the lives of caregivers of the patients. Treudley (1946) [2] referred to BOC as the resultant effect on the caregivers tendering psychiatric patients. The family burden has been defined by Dillehay and Sandys [3] as a "psychological state produced by the combination of physical work, emotional pressure, social restrictions, and economic demands arising from taking care of a patient as well". Psychiatric disorders, and especially violence, have a major impact on quality of life [4-6] and it reduces the quality of life [7]. Reduction in the QOL of relatives of schizophrenic patients has been related to the burden they undergo and this, in turn, impacts caregiver’s health [8-10]. The World Health Organization (WHO) states caregiver burden as the “the emotional, physical, financial demands and responsibilities of an individual’s illness that are placed on the family members, friends or other individuals involved with the individual outside the health care system [1]. Social, emotional, behavioral, and limitations on personal life are the by-product for the person who works as a caregiver of psychiatric patients [11]. Conceptualized into two distinct components BOC can be (objective and subjective). Former is meant to show its effects on the household such as taking care of daily tasks, whereas the latter reflects itself on the extent to which the BOC is perceived by the caregivers [12].
Quality of Life (QOL): QOL is a multi-faceted concept covering a wide variety of an individual’s life ranging from emotional health to daily routine tasks and has been discussed in detail by [13]. Though previously because of good medical research more focus has been on QOL of on schizophrenia patients rather than their caregivers. But a study by [14] suggested that informal and formal caregivers are being considered as a valuable component of an integral treatment for patients, thus their QOL and burden must be evaluated.
Knowledge: Concrete objective Information vis-à-vis attitudes and their functioning is of interest both theoretically and practically. No theory of social behavior can be complete without the incorporation of attitude functioning, and it is doubtful that complex social behavior can be predicted without knowledge of attitude. To study attitudes requires that they are measured in some way [15]. To assess knowledge, confidence, and attitude towards mental health for nurses and the effects of training a study was conducted [16]. The study concluded that confidence in nurses augmented after receiving mental health training. Nurses felt positive towards their role in treating depressed patients [16]. Thus, it can be concluded that an increase in the level of knowledge lessens the BOC, and which in turn increases the QOL so knowledge, therefore, moderates the relationship between BOC and QOL
Gender: Many socio-demographic and psychological variables are affected by BOC, but the gender of the caregiver has the most significant role to play in this caregiving gamut. A large portion of the caregiver’s responsibilities rest on the shoulders of females [17], and caregivers who are younger experience greater burden [18]. Studies in the eighties in the United States pointed to the fact that there is a predominance of females as caregivers, but at the same time 20% and 33% of the caregivers are men but with elderly patients [19]. On gender differences, Yee et al. [20] in their work extracted data on caregiver-burden from 17 of the 30 studies they had included in their review. Most of these studies showed that female caregivers experienced higher levels of BOC than males.
Correlation between the perceived BOC of caregivers and some socio-demographic variables was elaboratively studied by Thara et al. (1998) [21]. Jafri et al. (2018) studied the relation between BOC and QOL of caregivers for hemodialysis patients and found a positive relation between BOC and QOL [22]. Therefore, it is recommended to pay more attention to the needs of caregivers and provide equip them with proper knowledge. Another study posited that patient care education (i.e. knowledge) decreases BOC and increases QOL of the caregivers of patients Hekmatpou et; al (2019) [23].
From the foregoing review of the literature, one can conclude that BOC affects the QOL of the caregivers as a whole and as such provides a raison d’être for capitalizing on the socio-demographic and related variables affecting caregivers of Schizophrenic patients. Moreover, we see some studies also suggest that knowledge moderates the relation between BOC and QOL (i.e. the more knowledge of the caregiver the lesser burden on him/her which positively affects their quality of life), and this holds better for female care-givers than their male counterparts. The authors could not come across any study in the literature that simultaneously studied the interaction of gender and knowledge on BOC and QOL at the same time. The results of the current study would facilitate enhancing the quality of life of both the mentally ill, and their caregivers.
The method section elaborates on the methodology adopted to address the objectives of the study. In the results section, all statistical results with relevant graphs are presented. Discussion section thoroughly discusses the implications of the results. Conclusion section briefly concludes the study followed by future implications.
Moderated moderation in the statistical literature is also commonly known as a three-way interaction. For the present study knowledge of the caregiver will be studied as a moderator between the relation of QOL and BoC. Moreover, the differential effect of gender will be studied as a moderated moderator of Knowledge on the relationship between QOL and BoC. Though the initial work on moderation and mediation was implicitly explained by Baron and Kenny (1978) but the idea was extended on a bigger canvas and further chiseled by Dr. Andrew in his pioneering work on contingency framework particularly designed for dealing with problems related to organizational behavior. But the frameworks suggested by Andrew (2013) can be extended to any field of study dealing with contingency frameworks – moderation, mediation, and their variations. The framework that suited our study was model 3 and the relevant diagrams are shown in Figure 1. There is moderation of M on the relationship between X and Y i.e. there is an interaction between M and X to predict Y but there is also W which moderates the relationship between M, X, and Y and this amounts to a three-way interaction between X, W, M and also all two-way interactions. The relationship between study variables is depicted well in the lower panel of Figure 1. In the current study, our first moderator M = knowledge and second moderator W = gender, whereas QOL is treated as the dependent variable (Y) and BOC is the explanatory variable (X). Thus, in the present study, we propose to establish that knowledge moderates the relationship between BOC and QOL, but this relationship is overall moderated by gender. In simple words, it can be said that if the level of knowledge increases the BOC decreases, and QOL increases but this relationship is more evident in females than in male caregivers. In the ensuing sections, we will like to establish moderated moderation of Gender and Knowledge on the relationship between BOC and QOL.
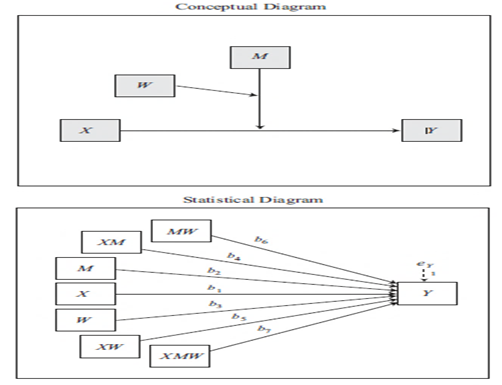
Source: Model Templates for PROCESS for SPSS and SAS c 2013 Andrew F. Hayes [24]
The aim of the Study:
To assess the moderated moderation effect of gender and knowledge levels on the relationship between BOC and QOL.
Methods
Quantitative cross-sectional design was used to address the objectives of the study. Relevant data were collected from five private hospitals in Jeddah having psychiatric department catering for schizophrenic patients. Hospital administration was briefed about the aims and objectives of the study with the undertaking that a copy of the published paper and results inferred shall be conveyed to them. The data was collected during working days for three consecutive months.
Taking care of the patient and being 18 years old or above with the diagnosis of schizophrenia; those who can understand both the Arabic and English languages; also spending a lot of time and emotions in the care of the patient.
Disobliging caregivers and not living with the patient for the last 12 months. Caregivers were excluded if they were involved in caring for more than one person with a diagnosed mental health problem.
The instrument for collecting data had two parts. Part I covered the demographic characteristics of the respondents about gender, age, academic qualification, relation with the patient, employment status, marital status, income, and the number of hours of conversation with the patient. Part II covered the aspects of Knowledge, BOC, and QOL.
A snow-balling sampling technique was used to collect the required information from 150 caregivers. The care gives were assured about their anonymity and convinced them about the nature of research and its implications. Descriptive analysis of the study variables along with their correlations and inferential analysis supplemented by relevant scatter plots exhibiting moderations among the study variables have been produced. For studying the moderated moderation, model 3 of Andrews (2013) is used. All results were calculated using an adds on known as “process” developed by Andrews (2013) which can be customized on SPSS ver 22.
Results
Table-1 exhibits descriptive information about the socio-demographic characteristics of the entire sample. In the sample of 150, majorities (65.3%) of the caregivers were females with less than 30 years of age. The concept of family burden is often a 'gendered' notion, with the lion's share of primary caregiving being provided by female relatives [27] In the present study, 65.3% of the caregivers were women. More than three-fourth of the caregivers were educated with almost 50% having studied up to secondary level. 28.7% were employed and 71% were unemployed. More than 70% of the caregivers were to some degree related to the patient and less than one-third (27.3%) were not related to the patients. More than one-third (38.7%) of the caregivers were married. More than one-third (35.3%) of patients had more than 4 family members living with him.
Table 1: Socio-demographic characteristics of the Caregivers (N=150)
|
|
Count |
% |
|
|
Gender |
Male |
52 |
34.7% |
|
|
Female |
98 |
65.3% |
|
Age |
< 30 |
80 |
53.3% |
|
|
> 30 |
35 |
23.3% |
|
|
> 40 |
27 |
18.0% |
|
|
> 50 |
8 |
5.3% |
|
Education |
Not Educated |
13 |
8.7% |
|
|
Primary |
23 |
15.3% |
|
|
Secondary |
76 |
50.7% |
|
|
Graduate |
38 |
25.3% |
|
Relationship with Patient |
No Relation |
41 |
27.3% |
|
|
Spouse |
21 |
14.0% |
|
|
Parents |
23 |
15.3% |
|
|
Offspring |
12 |
8.0% |
|
|
Siblings |
25 |
16.7% |
|
|
Other Relatives |
28 |
18.7% |
|
Marital Status of the Caregiver |
Married |
58 |
38.7% |
|
|
Unmarried |
29 |
19.3% |
|
|
Single |
51 |
34.0% |
|
|
Divorce |
12 |
8.0% |
|
Patient Care Providers Job |
Working |
43 |
28.7% |
|
|
Not Working |
107 |
71.3% |
|
Number of Family Members Living with the Patient |
Don't Know |
36 |
24.0% |
|
|
1-2 |
28 |
18.7% |
|
|
2-4 |
33 |
22.0% |
|
|
More Than 4 |
53 |
35.3% |
Tables 2 – 5 deal with inferential statistics of the study variables. To test whether the levels of knowledge for the caregivers in our sample differ or not, it is witnessed in Table 2 that the levels of knowledge do differ significantly (χ2= 76.96 (2) has p-value < 0.01) with a majority of the caregivers (65.3%) having a low level of knowledge. Table 3 shows the test results for mean levels of QOL and BOC. The mean values are tested against the test value of 3 as this is the neutral value of the Likert scales for both QOL and BOC. For QOL, the mean level is different (< 3) from than the neutral value and that this difference is significant [t (149)= -5.344 ; p < 0.01] and for BOC the mean level is different (> 3) from than the neutral value and that this difference is significant [t (149)= 19.002; p < 0.01]. Summing up the results from Tables 2 and 3, it is posited that caregivers are experiencing more BOC and less QOL and that three levels of knowledge differ significantly.
Table 2: Chi-Square Test for three Knowledge Levels
|
|
N |
% |
Chi-Square (χ2) |
|
|
Knowledge |
1 |
98 |
65.3% |
76.960 |
|
|
2 |
40 |
26.7% |
(df =2) |
|
|
3 |
12 |
8.0% |
Sig (0.000) |
|
Table 3: One-Sample Test (QOL and BOC) |
||||||||
|
|
|
|
Test Value = 3 |
|||||
|
Mean |
Std. Error Mean |
t |
df |
Sig. (2-tailed) |
Mean Difference |
95% C.I |
||
|
|
|
|
|
|
|
Lower |
Upper |
|
|
QOL |
2.5704 |
0.0803 |
-5.344 |
149 |
.000 |
-.4296 |
-.5885 |
-.2708 |
|
BOC |
3.9318 |
.04904 |
19.002 |
149 |
.000 |
.9310 |
.8349 |
1.0287 |
Table 4 though provides bivariate analysis but deals with three study variables simultaneously (i.e. QOL & BOC vis-à-vis gender ) values in the same row of Table 4 not sharing the same subscript are significantly different at p < .05 in the two-sided test of equality for column means. Now regarding QOL, there is no significant difference between gender means i.e. both male and female caregivers are experiencing low QOL and there is no difference in their mean levels of experiencing low QOL. However, as far as BOC is concerned, female caregivers undergo more BOC (mean = 4.01) than their male counterpart (mean = 3.79) and this difference is significant at p < .05 since the two mean values for BOC in the second row of Table 4 do not share the same subscript. Table 5 like Table 4 also provides bivariate analysis and deals with three study variables simultaneously (i.e. QOL & BOC vis-à-vis knowledge) values in the same row of Table 5 not sharing the same subscript are significantly different at p < .05 in the two-sided test of equality for column means. Regarding BOC, there is no significant difference between means of knowledge level i.e. whether the level of knowledge is low (1) or high (3), the BOC remains high. But, as far as QOL is concerned higher, mean levels of knowledge result in higher QOL and that this difference is significant at p < .05 since the three mean levels of knowledge in the first row of Table 5 do not share the same subscript. Summing up the results of Table 4 and Table 5, it can be said that there is a differential effect of gender on BOC but not on QOL and that there is a differential effect of knowledge on the QOL but not on BOC.
Table 4: Gender vs QOL & BOC
|
|
Gender |
|
|
Male |
Female |
|
|
Mean N=52 |
Mean N=98 |
|
|
Quality of Life |
2.68a |
2.51a |
|
Burden of Care |
3.79a |
4.01b |
Table 5: Knowledge vs QOL & BOC
|
|
Knowledge |
||
|
1 |
2 |
3 |
|
|
Mean N=98 |
Mean N=40 |
Mean N=12 |
|
|
Quality of Life |
2.38a |
2.88b |
3.07a,b |
|
Burden of Care |
3.95a |
3.67a |
3.60a |
Nunnally (1978) posited that any value of coefficient α (α > 0.70) is an indication of substantial item homogeneity and suggests that the sampling sphere has been adequately captured [28]. Cronbach's α for the study variables of the present study are exhibited in Table 6 ranging from (0.780 -0.940) thus indicating a good structure of the sub-scales.
Table 6: Inter-item Consistencies (Cronbach’s ‘α’)
|
Study Variables |
No of Items |
Cronbach’s ‘α’ |
|
Knowledge |
25 |
0.780 |
|
Burden of Care |
6 |
0.817 |
|
Quality of Life |
18 |
0.940 |
Table 7 studies the association among the study variables. It is seen that there is a significant negative correlation between BOC and QOL [r(150)=-0.436, p < 0.01] i.e. for lower values of QOL an increase is witnessed in the BOC. Also, there is a significant negative correlation between knowledge and BOC [r(150)=-0.220, p < 0.01] which means that as the levels of knowledge of caregivers increase, the BOC of caregiver decreases and same is witnessed in the right-hand panel of Figure 2. Gender and BOC are significantly positively correlated [r(150)= 0.175, p < 0.05] indicating that female caregivers experience more BOC than the male caregivers, and the same is also witnessed in the left-hand panel of Figure 2. The correlation results support the apriori expectation that caregivers with high levels of knowledge will have low perceived BOC and high QOL and that female care-givers experience higher BOC.
Table 7: Pearson’s Correlations among Study Variables (N=150).
|
|
BOC |
QOL |
Knowledge |
|
|
QOL |
Correlation |
-.436** |
|
|
|
Knowledge |
Correlation |
-.220* |
.236** |
|
|
Gender |
Correlation |
.175* |
-.084 |
-.150 |
**. Correlation is significant at the 0.01 level (2-tailed)
*. Correlation is significant at the 0.05 level (2-tailed)
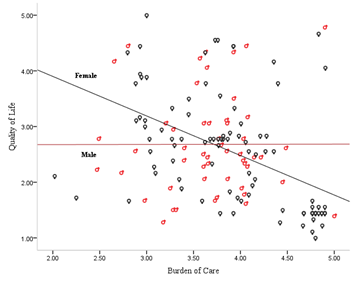
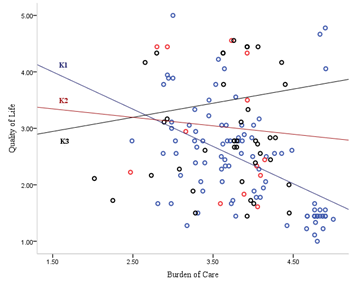
Figure 2: The moderating effects of gender and knowledge on BOC and QOL.
Moderated moderation is also known as three-way interaction. Tables 8-12 establish the proposed moderated moderation among the study variables. Overall variation accounted by gender, knowledge, and QOL as shown in Table 8 is 28.54% (R2 =0.2854) i.e. approximately 29% of the variation in the model is explained by gender, knowledge, and QOL and that this contribution is significant F(7,142) = 8.105, p < 0.001. When studying moderation, one must look at the significance of the interaction terms. All two-way interactions and three-way interaction in Table 9 are significant at p < 0.05. Table 10 shows the contribution of the variation (3.64%) in the model due to three-way interaction and its significance [F(1,142)=7.2384, p < 0.01 R2-change= 0.0364]. This supports the proposed relationship of moderated moderation i.e. knowledge moderates the relationship between QOL, and BOC and this moderation are overall moderated by gender. Table 11 exhibits the conditional effect of QOL on BOC at different values of moderators. There is no significant effect of male caregiver's knowledge levels on the relationship between QOL and BOC but for female caregivers, the significant negative differential effect of knowledge on the relationship between QOL and BOC is witnessed. The said differential effect of female knowledge levels is more for a low and medium level of knowledge and less for a higher level of knowledge. This may be since fewer data (N=8) were available for higher levels of knowledge. Figure 3 exhibits the moderated moderation relation of gender and knowledge on QOL and BOC. The upper panel of Figure 3 shows three levels of knowledge of male caregivers the three lines through cross each other but run somewhat parallel to BOC which points to the fact that with the increase in the knowledge levels there is no effect on BOC but in the lower panel significant decrease in the BOC is witnessed with the increase in the knowledge level. Summarizing the results, it can be posited that though an increase in the level of knowledge does decrease BOC this is more apparent in the female caregivers than male caregivers and this decrease in BOC, in turn, increases the QOL of the caregivers. Data for producing Figure 3 are appended in Appendix 1 to be copied and pasted in the script window of SPSS and run the procedure.
Table 8: Omnibus Test (N=150)
|
R |
R2 |
MSE |
F |
df1 |
df2 |
p |
|
.5342 |
.2854 |
.3343 |
8.105 |
7.00 |
142.00 |
.0000 |
Table 9: Model Coefficients
|
|
Coefficients |
se |
t |
p |
LLCI |
ULCI |
|
Constant |
0.4180 |
1.2815 |
.3262 |
.7448 |
-2.1152 |
2.9512 |
|
Knowledge |
1.5083 |
.7557 |
1.9960 |
.0478 |
.0145 |
3.0022 |
|
QOL |
1.0886 |
.4564 |
2.3853 |
.0184 |
.1864 |
1.9907 |
|
QOL x Knowledge |
-0.5045 |
.2541 |
-1.9851 |
.0491 |
-1.0068 |
-.0021 |
|
Gender |
2.8556 |
.7321 |
3.9003 |
.0001 |
1.4083 |
4.3029 |
|
QOL x Gen |
-0.9238 |
.2619 |
-3.5274 |
.0006 |
-1.4415 |
-.4061 |
|
Knowledge x Gen |
-1.2723 |
.4547 |
-2.7980 |
.0059 |
-2.1712 |
-.3734 |
|
QOL x Knowledge x Gen |
0.4084 |
.1518 |
2.6904 |
.0080 |
.1083 |
.7084 |
Table 10: R-square increase due to three-way interaction.
|
|
R2-change |
F(1,df2) |
df2 |
p |
|
QOL x Knowledge x Gender |
.0364 |
7.2384 |
142.0000 |
.0080 |
Table 11: Conditional effect of QOL on BOC at different values of the moderator(s).
|
|
Gender |
Knowledge |
Effect |
se |
t |
p |
LLCI |
ULCI |
|
Male |
1 |
1.0000 (low) |
.0687 |
.1201 |
.5718 |
.5683 |
-.1687 |
.3061 |
|
|
1 |
1.4267(medium) |
.0277 |
.0956 |
.2894 |
.7727 |
-.1613 |
.2167 |
|
|
1 |
2.0649(high) |
-.0337 |
.1032 |
-.3261 |
.7448 |
-.2377 |
.1704 |
|
Female |
2 |
1.0000(low) |
-.4467 |
.0721 |
-6.1934 |
.0000 |
-.5893 |
-.3041 |
|
|
2 |
1.4267(medium) |
-.3135 |
.0602 |
-5.2114 |
.0000 |
-.4324 |
-.1946 |
|
|
2 |
2.0649(high) |
-.2142 |
.0866 |
-2.4734 |
.0492 |
-.2854 |
-.0569 |
values for knowledge moderator are the mean and plus/minus one SD from mean.
values for gender moderators are the two values of the moderator.
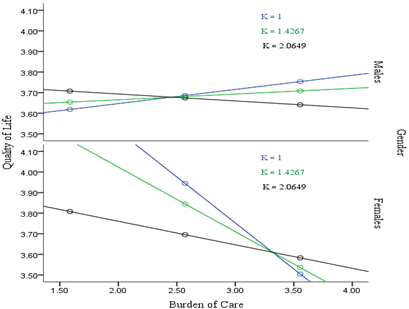
Figure 3: Showing Moderated Moderation of gender and knowledge on the relation between BOC and QOL.
Discussion:
The present study was undertaken to assess the knowledge about schizophrenia among caregivers of Schizophrenic patients in Jeddah, Saudi Arabia. Moreover, the effect of Gender on the moderating relationship between Knowledge and BOC and QOL. It is the first study of its kind which applied the contingency framework of moderated moderation on psychological study variables. The analysis was done for the association between burden and socio-demographic characteristics with special emphasis on gender differences. The results revealed that there was a significant difference in the burden of care among male and female caregivers with female caregivers feeling more BOC than male caregivers. The correlation of BOC with the socio-demographic characteristics reveals that as the gender is shifted from males to females BOC also increases, hence, we can say that females feel more burden than their male counterparts. BOC had a negative significant correlation with knowledge about schizophrenia, a positive significant correlation with QOL. QOL of the caregivers was on average less than what the caregiver had thought, as the overall mean of QOL was 2.57. Han et al. (2014) found that the relationship between marital status and QOL may vary depending on age and gender [29]. Results revealed that there was a significant positive correlation between knowledge and QOL i.e. as the knowledge of the caregivers increases, the QOL of caregiver increases. This points to the fact that as the knowledge of the caregivers about Schizophrenia increases likewise his/her QOL increases. In a nutshell, it can be posited that female caregivers possessing more knowledge will feel less BOC and have better QOL. Our study found that the impact of the caregiving burden on caregivers’ QOL is high, which is in line with other studies [26]. The findings of the present study are consistent with other Indian and Western studies; see Caqueo et al. (2009) and Srivastava et al. (2016) [30, 31]. Keeping in view the wide implications of the present research, it is suggested that psychiatrists, psychologists, and other health workers not only assist the patients but also give proper attention to the caregivers.
Conclusion:
In the present study, significant gender differences coupled with the differential effect of knowledge on the relation between BOC and QOL are found, these will have major implications for the development of gender-specific caregiver interventions. This study will provide the much-needed stimulus to the administration in the health sector to frame such social policy recommendations which will improve the plight of female caregivers. It is for this very reason that there is a need for continuing research in this area. The author concludes the present study with the quotation from Struening et al. (2001) “It seems that the current prosperity of the United States offers a realistic fiscal basis for change and improvement in mental health services. However, public attitudes and beliefs and related behaviors that we have reviewed here offer formidable impediments to change and progress. The important question remains: We have the resources, but do we have the will?” [32]
Ethics:
This article does not contain research involving humans or animals.
Acknowledgment:
The authors recognize the valuable suggestions of Dr. Nawal G. Alghamdi for improving the manuscript.
Financing:
This study did not have any financial support from third parties.
Author’s Contribution:
Conceived/material, instrument, data collection, and discussion/implications were done by Areej, review of the literature, analyses of the data/selection of appropriate statistical tools, and result reporting were done by K Khan.
Conflict of Interests:
The authors claim there is no conflict of interest.
References
Appendix ‘A’
SPSS code for Generating Figure 3
Model = 3
Y = QOL
X = BoC
M = know
W = Gen
DATA LIST FREE/ BurdenofCare Gen kl QOL.
BEGIN DATA.
1.5858 1.0000 1.0000 3.6185
2.5704 1.0000 1.0000 3.6861
3.5549 1.0000 1.0000 3.7537
1.5858 1.0000 1.4267 3.6541
2.5704 1.0000 1.4267 3.6814
3.5549 1.0000 1.4267 3.7086
1.5858 1.0000 2.0649 3.7075
2.5704 1.0000 2.0649 3.6743
3.5549 1.0000 2.0649 3.6412
1.5858 2.0000 1.0000 4.3844
2.5704 2.0000 1.0000 3.9445
3.5549 2.0000 1.0000 3.5047
1.5858 2.0000 1.4267 4.1535
2.5704 2.0000 1.4267 3.8448
3.5549 2.0000 1.4267 3.5361
1.5858 2.0000 2.0649 3.8081
2.5704 2.0000 2.0649 3.6956
3.5549 2.0000 2.0649 3.5832
END DATA.
GRAPH/SCATTERPLOT=BurdenofCare with QOL BY kl/PANEL ROWVAR=Gen

