Pharmacophore an International Research Journal
The Result of Surgical and Combined Treatment of Patients with Acromegaly
Sameh R.A. Ibrahim1*, Gennady Chmutin1, Koval K.V.1, Mekhaeel M.Sh.1, Al Awaida Wajdy2, Al-bawareed O.A.3
|
|
|
ABSTRACT
Purpose of the work: to evaluate the results of surgical and combined (medical and surgical) treatment of patients with acromegaly. Materials and methods: 121 patients with a diagnosis of acromegaly (81 women (66.94%); 40 men (33.06%) were operated on. All patients were divided into 4 groups, comparable in terms of gender and age parameters: group 1 consisted of 30 patients (mean age of 46.89 ± 2.34 years) who underwent surgical treatment; group 2 included 30 patients (mean age of 47.01 ± 2.35 years) who received preoperative drug treatment with somatostatin analogues and underwent surgical treatment; group 3 consisted of 30 patients (mean age of 45.02 ± 2.25 years) who underwent surgical treatment and received postoperative drug treatment with somatostatin analogues; group 4 included 31 patients (mean age of 44.9 ± 2.25 years) who underwent surgical treatment and received drug treatment with somatostatin analogues both in the preoperative and postoperative periods. Observation of patients was carried out in the postoperative period (on the 7th day), as well as after 6 and 12 months. Results: In most cases, when using these methods of surgical intervention, a significantly greater number of total tumor resection was performed. The largest number of patients, in whom remission was registered after the surgical treatment, was observed after 12 months of observation (50% and 51% of cases, respectively, for each type of surgery). Pre- and postoperative administration of drug treatment (somatostatin analogs) increases the frequency of "remission in the entire group" up to 27.4%, reaching 96.7% in group. Conclusion: The use of combined methods of treatment contributed to the achievement of remission in a greater number of cases compared with only surgical treatment. Moreover, the largest number of patients who reached a state of remission was observed 12 months after the start of therapy.
Keywords: acromegaly, remission, somatotropic hormone, insulin-like growth factor 1, transsphenoidal resection.
Introduction
Acromegaly is a chronic disease characterized by hypersecretion of growth hormone (somatotropic hormone – STH), mainly caused by a pituitary adenoma [1-3]. According to the medical literature, the prevalence of the disease ranges from 2.8-13.7 cases, and the annual incidence is 0.2-1.1 cases per 100,000 people; however, the actual incidence is likely much higher [2]. Growth hormone stimulates the synthesis of insulin-like growth factor 1 (IRF-1), which is formed in the liver, as well as locally in peripheral tissues under the influence of STH [4-6].
Hypersecretion of STH mediates most of the phenotypic features and metabolic effects. In addition to changing the patient's appearance, characteristic features are metabolic disorders, pathological changes in the motor, cardiovascular, and respiratory systems.
The clinical picture in acromegaly depends not only on changes that are caused by an increase in the level of STH but also on the local effect of the tumor itself on the surrounding structures. In most cases, this is manifested primarily by visual and oculomotor disorders.
Transsphenoidal resection of the pituitary adenoma is usually the most commonly used technique in practice. Successful surgery ensures an immediate reduction in growth hormone levels and provides tumor tissue for diagnostic and prognostic purposes. However, not all patients achieve remission after surgery, and acromegaly treatment is often multimodal [7, 8]. Decreased preoperative growth hormone values, small tumor size, and extrapseudocapsular resection are factors associated with a higher postoperative remission rate, while a lower remission rate is observed in macroadenomas and tumors affecting the cavernous sinus and parasellar region. STH <1 ng/ml during the first 3 days is a positive predictor of remission [9-11]. Pharmacological agents available for the treatment of acromegaly include somatostatin receptor ligands, GH receptor antagonists, and, in selected cases, dopamine agonists [12].
Radiation therapy remains the third method in the treatment algorithm for acromegaly and is usually considered in cases of large residual (or enlarging) tumor after surgery, and if drug therapy is ineffective or poorly tolerated. At the present stage of the development of radiation therapy in the treatment of this pathology, great importance is attached to stereotaxic methods, stereotaxic radiosurgery (SRS), and fractionated stereotaxic radiation therapy (FSRT), which provide a more accurate and higher dose of radiation to the target tumor and limit the radiation of adjacent normal structures.
Purpose of the work:
To evaluate the results of surgical and combined (medical and surgical) treatment of patients with acromegaly.
Materials and methods
121 patients with a diagnosis of acromegaly (81 women (66.94%); 40 men (33.06%)) were operated on.
The patients’ mean age was 45.07 ± 2.25 years. The disease duration from the onset of clinical manifestations to surgical treatment averaged 5.5 ± 2.4 years (from 8 months to 20 years).
A comprehensive examination was performed, which consisted of an examination by neuroendocrinologist, neurosurgeon, ophthalmologist, and otorhinolaryngologist. The following laboratory tests were carried out: general analysis of blood and urine, biochemical analysis of blood, etc. Using the radioimmune method, the tropic hormones of the pituitary gland (prolactin, somatotropic hormone, adrenocorticotropic hormone, thyroid-stimulating hormone, follicle-stimulating hormone, luteinizing hormone), as well as hormones that are produced by the peripheral endocrine glands (cortisol, testosterone, free T4, and others) were identified in the blood. In order to confirm this diagnosis, an additional study of insulin-like growth factor-1 (IGF-1) was performed. In the presence of clinical and biochemical parameters in patients of the group under study, the presence of a pituitary tumor was confirmed by MRI.
All patients were divided into 4 groups, comparable in terms of gender and age parameters: group 1 consisted of 30 people (mean age of 46.89 ± 2.34 years) who underwent surgical treatment; Group 2 included 30 people (mean age of 47.01 ± 2.35 years) who received preoperative drug treatment with somatostatin analogues and underwent surgical treatment; Group 3 consisted of 30 people (mean age of 45.02 ± 2.25 years) who underwent surgical treatment and received postoperative drug treatment with somatostatin analogues; Group 4 included 31 people (mean age of 44.9 ± 2.25 years) who underwent surgical treatment and received drug treatment with somatostatin analogues both in the preoperative and postoperative periods.
All patients underwent surgery, which was carried out using transnasal transsphenoidal access.
When performing the surgical intervention, different approaches were used: endoscopic ones were applied to most of the patients (in 60.33%); the microscopic technique was used in 39.67% of cases.
According to the consensus [13], the main criteria of acromegaly remission included: the absence of clinical signs of activity, basal STH <2.5 ng/ml, minimum STH level against the background of OGTT <1 ng/ml (2.7 mU/L), a normal level of IGF-1 according to gender and age [13, 14].
Thus, remission was diagnosed in patients with normalization of hormonal parameters in terms of such indicators as: basal level of STH, STH in OGTT, and IGF-1.
Observation of patients was carried out in the postoperative period (on the 7th day), as well as after 6 and 12 months.
The statistical significance of the results obtained was assessed using descriptive statistics methods. The following analysis methods were used: correlation, regression, and variance. In addition, the diagnostic significance of the criteria under study was calculated. The results obtained were presented as mean (M) and standard error of the mean (m). Wilcoxon's test was used to assess differences. Results with p<0.05 were considered statistically significant.
Results
Table 1 presents comparative characteristics of surgery radicality degree in patients in the early postoperative period, depending on the type of surgery.
Table 1. The nature of surgery radicality degree in patients in the early postoperative period, depending on the type of surgery.
|
Radicality of the excision |
Surgical method |
|
|
Microscope Abs (%) |
Endoscope Abs (%) |
|
|
Total excision |
40 (83,3%)* |
66 (90%)* |
|
Subtotal excision |
6 (12,5%) |
6 (8,2%) |
|
Partial excision |
2 (4,2%) |
1 (1,8%) |
|
Total |
48 (100%) |
73 (100%) |
* р<0.05 – the statistical significance of differences in characteristic within each of the surgical groups
The presented data indicate that in most cases, when using these methods of surgical intervention, a significantly greater number (p<0.05) of total tumor excision was performed. At the same time, a greater number of people who underwent total tumor excision were recorded in the endoscopy group (90% versus 83.3% in the group using microscopic operations) (p> 0.05).
This fact may be associated primarily with the fact that when using endoscopic technology, a larger angle of view is noted. In addition, better illumination of the operating field and the possibility of performing manipulations that are not limited to the nasal port are used. This, first of all, makes it possible to perform more radical interventions (using intraoperative imaging and subsequent MRI control) with total excision of the tumor in more than 90% of cases.
Comparative characteristics of remission onset in patients, depending on the type of surgery, are presented in Table 2.
Table 2. Comparative characteristics of remission onset in patients depending on the type of surgery
|
Timing of remission |
Microscope |
Endoscope |
||||
|
|
Abs. |
% of the group |
% of cohort |
Abs. |
% of the group |
% of cohort |
|
postoperatively |
7 |
17,5 |
14,6 |
12 |
18,2 |
16,4 |
|
6 months |
13 |
32,5 |
27,1 |
20 |
30,3 |
27,4 |
|
12 months |
20 |
50* |
41,7# |
34 |
51,5* |
46,6# |
|
Total in cohort |
48 |
|
100 |
73 |
|
100 |
|
Total in remission |
40 (83,3%) |
66 (90,4%) |
||||
* Р<0. 05 confidence of characteristic differences within each of the groups of surgical intervention (% of the group) # р<0.05 confidence of characteristic differences within each of the groups of surgical intervention (% of cohort)
According to the data obtained, it can be noted that the largest number of people in whom remission was recorded after the surgical treatment was observed after 12 months of observation (50% and 51%, respectively, for each type of surgery) (p<0.05).
One year after surgery, there was no hormonal remission of the disease in 15 patients (12.39%); however, their condition was regarded as the onset of improvement according to clinical and hormonal parameters.
The general condition of these patients was assessed as good since it was accompanied by a decrease in the level of growth hormone to normal values. However, in the early postoperative period and 3 months after the operation, there were no signs of hormonal remission of the disease. The choice of further treatment tactics was associated with the use of other methods of therapeutic action (in particular, the use of radiation therapy).
The main reason for the unsatisfactory result in the case of surgical treatment was the partial excision of the tumor due to its invasion of the cavernous sinus.
The negative effect of surgery, in some cases, was due to tumor infiltration into the dura mater.
Figure 1 shows the number of people in each of the 4 groups under study (as a percentage) who achieved remission after undergoing the applied treatment method for each of the groups during the observation period.
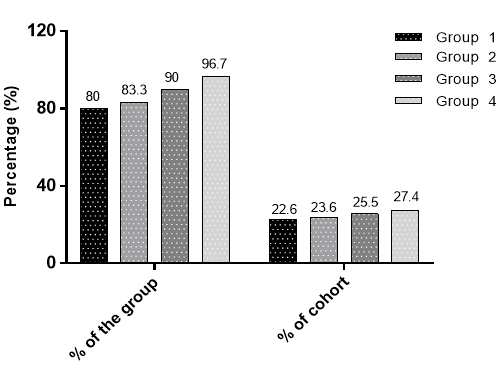
Figure 1: Comparative characteristics of the number of people in each of the 4 groups under study (in percentage), who achieved remission after undergoing the applied treatment method for each of the groups after 12 months.*р<0.05 the statistical significance of characteristic differences between groups
The presented data indicate that pre- and postoperative administration of drug treatment (somatostatin analogs) increases the frequency of "remission in the entire group" to 27.4%, reaching 96.7% in the 4th group under study (* p <0.05)
When comparing the results in the groups with preoperative drug intake of somatostatin analogues and with only surgical treatment, only a slight prevalence of remission frequency after a year was noted in group 2 (23.6% versus 22.6%). This circumstance is primarily due to the fact that there were patients who were obviously more resistant to treatment. In these patients, biochemical remission of the disease was not achieved while taking somatostatin analogues. In this regard, no statistical difference was obtained, p> 0.05.
In group 3 with postoperative prescription of drug treatment to patients who did not have the disease remission in the postoperative period, the possibility of its development in 25.5% of patients increased, reaching 90%, which is the maximum value in the group.
Comparative characteristics of the timing of remission onset in patients of groups under study (in percentage) are presented in Table 3.
Table 3. Comparative characteristics of the timing of remission onset in patients of groups under study
|
Timing of remission |
Group 1 (n=30) Abs., % |
Group 2 (n=30) Abs., % |
Group 3 (n=30) Abs., % |
Group 4 (n=31) Abs., % |
|
postoperatively |
4 (13,3) |
6 (20) |
3 (10) |
6 (19,4) |
|
6 months |
9 (30) |
8 (26,7) |
9 (30) |
10 (32,3) |
|
12 months |
11 (56,7)* |
12 (53,3)* |
15 (60)* |
13 (48,3)* |
|
Total |
30 (100) |
30 (100) |
30 (100) |
31 (100) |
|
Remission |
24 (80) |
25 (83,3) |
27 (90) |
29 (96,7) |
*р <0.05 the statistical significance of the characteristic differences within groups The presented data indicate that the largest number of patients, in whom remission was registered, occurred after 12 months (p <0.05).
The Discussion of the Results
The problem of treating acromegaly is a rather complex and urgent issue in modern medical practice. This is primarily due to the fact that in most cases this pathology is associated with the development of a pituitary tumor and requires surgical intervention, which is confirmed by medical literature data [15, 16]. Another problem is the achievement of remission in the postoperative period (according to the hormonal status) [17, 18]. This fact determines the most frequent use of combined treatment methods to increase the possible percentage of cases of improvement after 6 and 12 months. Many researchers have noted that the combination of surgical treatment with drug therapy in the pre- and postoperative periods often increases the frequency of remission in patients, which is most pronounced after 12 months [19-21]. The results obtained in this study are consistent with the medical literature.
Conclusion
The use of combined methods of treatment (surgical treatment + drug therapy in the pre- and postoperative periods) contributed to the achievement of remission (according to hormonal levels) in a greater number of cases compared with only surgical treatment. Moreover, the largest numbers of patients, who have reached a state of remission, are observed after 1 year.
References


