Pharmacophore an International Research Journal
In 2022, the number of overweight children under the age of 5 was estimated at 37 million people. Although it was formerly thought to be an issue in wealthy nations, overweight people are becoming more common in low- and middle-income nations as well. Notably, obesity in children and adolescents has significant psychosocial effects; it impairs quality of life and academic performance and is exacerbated by discrimination, unfavorable attitudes, and bullying from others. To study the morphometric parameters of mesenteric, epididymal, retroperitoneal and the white adipose tissue under the skin in rats fed a high-fat diet. In rats on a standard diet, the specific gravity and average size of adipocytes of epididymal adipose tissue predominate. A high-fat diet causes all forms of adipose tissue, with a predominance of subcutaneous, to have a higher specific weight. An increase in the specific mass of visceral fat depots is associated with the predominance of large adipocytes. In subcutaneous adipose tissue in rats with a high-fat diet, small adipocytes predominate in comparison with adipose tissue of other localization.
Introduction
Overweight is a condition characterized by the presence of excess body fat [1]. Obesity is a complex chronic disease in which excessive accumulation of fatty tissues can negatively affect health [2]. Obesity can increase the risk of type 2 diabetes mellitus and cardiovascular diseases, have negative consequences for the state of the musculoskeletal system and reproductive function, and also increase the risk of developing certain types of cancer [3-5]. Obesity affects the quality of life, in particular sleep and mobility.
In 2022, the number of adults aged 18 and over who were overweight reached 2.5 billion, with over 890 million of those classified as obese. According to the data, 43% of adults who were 18 years old or older were classified as overweight. This percentage was divided into 43% for men and 44% for women. In contrast, in 1990, just 25% of adults who were 18 years old or older were considered overweight. The percentage of overweight people ranged from 31% in the WHO African and Southeast Asia regions to 67% in the Americas [6].
In 2022, approximately 16% of adults aged 18 and over worldwide were obese. Between 1990 and 2022, the prevalence of obesity more than doubled worldwide.
The anticipated global population of children under the age of 5 who are overweight in 2022 was 37 million individuals. The issue of overweight was formerly associated with affluent nations, but, it is now becoming more prevalent in low- and middle-income countries as well. The prevalence of childhood obesity in Africa has risen by nearly 23% since 2000, affecting children under the age of 5. In 2022, almost half of overweight or obese children under the age of 5 lived in Asian countries [7].
In 2022, there were 390 million overweight children and adolescents between the ages of 5 and 19 in the world. In children and adolescents aged 5-19, the prevalence of overweight (including obesity) has risen dramatically: from 8% in 1990 to 20% in 2022. This upward trend is similar among boys and girls: in 2022, 19% of girls and 21% of boys were overweight.
If in 1990 only 2% of children and adolescents aged 5 to 19 years (31 million people) were obese, then by 2022 this figure had increased to 8% (160 million people). Overweight and obesity occur when there is an imbalance between the amount of energy consumed through nutrition and the amount of energy expended through physical activity [8, 9]. Obesity is typically a complex condition resulting from a combination of environmental, psychosocial factors, and genetic susceptibility [10]. In some patients, one leading etiological factor of obesity can be identified (taking medications, the presence of diseases, reduced mobility, medical procedures, and monogenic disease/genetic syndrome) [11]. At the same time, the development of obesity is further facilitated by the lack of effective healthcare measures that allow the detection of cases of excessive weight gain and accumulation of adipose tissue in the early stages [12].
There is an increasing amount of data that contributes to understanding the health risks associated with overweight and obesity. In 2019, it is anticipated that 5 million fatalities were caused by non-communicable diseases such as cardiovascular diseases, diabetes, cancer, neurological disorders, chronic respiratory diseases, and digestive problems due to having a BMI that exceeded the recommended values [13-16].
Childhood and adolescent obesity has a direct impact on the health of young individuals and is linked to a higher risk and earlier onset of several non-communicable diseases, including type 2 diabetes mellitus and cardiovascular diseases [17]. Childhood and teenage obesity has severe effects on mental and social well-being. It can impact academic performance and overall quality of life. Additionally, it is worsened by the presence of unfavorable attitudes, discrimination, and bullying from others [18-20]. Obesity in childhood is associated with a higher likelihood of having non-communicable diseases in maturity. The obesity epidemic also has serious economic consequences [21]. In the absence of measures to address the problem, by 2030, the global costs associated with overweight and obesity will reach 3 trillion US dollars per year, and by 2060, they will exceed 18 trillion US dollars [22].
Lastly, the rise in obesity rates in low- and middle-income nations, particularly in those belonging to less affluent socioeconomic classes, gives a global character to this problem, although it was once considered typical only for high-income countries [23].
For many years, the World Health Organization (WHO) has recognized the need to urgently address the crisis caused by the spread of obesity.
WHO member states have approved the global nutrition objectives of the World Health Assembly aimed at curbing overweight among children, as well as the task of combating noncommunicable diseases, which is to stop the increase in the incidence of diabetes and obesity by 2025. They acknowledged the necessity to expedite international efforts in order to tackle the extensive and harmful issue of the dual burden of malnutrition [24].
During the seventy-fifth session of the World Health Assembly in 2022, Member States endorsed and ratified new guidelines pertaining to the prevention and treatment of obesity. They also accepted the WHO Plan to Accelerate Measures to Combat Obesity [25]. Since its implementation, the Acceleration Plan has established the essential political conditions to incentivize sustained transformation and has served as a platform for developing, coordinating, and prioritizing policies in this area, facilitating practical work in countries, as well as achieving real results and strengthening accountability at the national and global levels.
The prevalence of obesity is an epidemic in developed countries. Adipose tissue not only concentrates the main supply of energy substrates of the body but also has endocrine activity [26-28]. There are two main fat depots: subcutaneous and visceral [29]. Adipose tissue has different morphological and physiological characteristics based on its topographic location [30]. When overweight, the nature of its distribution affects the development of metabolic disorders. The amount of visceral adipose tissue is one of the important prognostic factors for the development of diseases associated with obesity [31].
Thus, the aim of this work was to study the morphometric parameters of mesenteric (MAT), epididymal (EAT), retroperitoneal (RAT), and subcutaneous (SAT) white adipose tissue of rats on a high-fat diet.
Materials and Methods
The studies were carried out on 20 white male rats of the Wistar line. The maintenance of laboratory animals and all manipulations to which they were subjected during quarantine and research corresponded to generally accepted rules of laboratory practice [32].
The animals were divided into 2 groups: Group 1 (control, 10 rats) received standard feed (the proportion of fat in the total caloric content of the feed was 11%) for laboratory rats and unlimited water. Group 2's animals, ten experimental rats, were fed a high-fat diet with unlimited water for eighteen weeks, with 32% of the feed's total calories coming from fat. By asphyxiating with CO2, the animals were taken out of the experiment.
Adipose tissue (mesenteric, epididymal, retroperitoneal, and subcutaneous) was separated, weighed on analytical scales by dissection, and its specific mass was computed once the body weight (the mass of adipose tissue per 100 g of rat body weight) was established. For morphometric examination, pieces of adipose tissue were fixed in 10% neutral buffered formalin (Biovitrum, Russia), dehydrated in isopropyl alcohol (Biovitrum, Russia), and poured into paraffin (Histomix, Russia). Sections 5-7 µm thick were made on the microtome MZP–01 (Technom, Russia), which were mounted on slides and stained with hematoxylin and eosin. The obtained micro–preparations were viewed in transmitted light on a Biomed-3M microscope (Russia) combined with a computer.
The average size of 500 fat cells was calculated for each group of animals, and the distribution of cells by size was approximated as a percentage of tiny cells (< 50 µm), medium cells (50-100 µm), and big cells (> 100 µm).
Statistical data processing was performed using the Statistics 6.0 software package using nonparametric statistical methods. The results obtained are expressed in the form of medians (Me), upper and lower quartiles (Q1–Q3). The differences were considered significant at p<0.05.
Results and Discussion
Obesity in rodents is considered as an increase in body weight due to fat depots compared with the control group. Criteria for assessing obesity in animals include such indicators as body weight gain, body mass index, and adipose tissue mass while measuring the total adipose tissue mass is a more sensitive indicator [33, 34].
As a result of the experiment, it was found that a high-fat diet in rats leads to an increase in animal body weight by 25% (p<0.01) (Table 1), which is due to an increase in the mass of fat depots, as evidenced by an increase in the specific mass of adipose tissue by 3 times (p<0.01). At the same time, the specific mass of mesenteric adipose tissue increased 2.1 times (p<0.01), epididymal – 1.6 times (p<0.01), retroperitoneal – 3.5 times (p<0.01), subcutaneous adipose tissue – 5.5 times (p<0.01), respectively, compared with the group of rats treated with standard a diet.
Table 1. Body weight and specific gravity of adipose tissue in the mesenteric, epididymal, retroperitoneal, and subcutaneous regions of rats fed a conventional, high-fat diet, Me (Q1- Q3)
|
Me indicators (Q ₁–Q₃) |
Experimental groups |
|
|
Group 1 (control) (n=10) |
Group 2 (experienced) (n=10) |
|
|
Body weight, g |
458 (442–478) |
578 (554–611) * |
|
specific mass of adipose tissue, g |
4.23 (4.11–4.34) |
12.63 (10.96–13.72)* |
|
specific mass MAT, g |
1.07 (1.06–1.1) |
2.25 (2.07–2.25)* |
|
specific mass EAT, g |
1.35 (1.22–1.39) |
2.18 (1.98–2.56)* |
|
specific mass RAT, g |
0.99 (0.97–1.04) |
3.38 (2.97–3.56)* |
|
specific mass SAT, g |
0.87 (0.85–0.92) |
4.87 (3.57–5.18)* |
Note: n is the number of animals in the group; * – p₂₋₁<0.01
It is known that in rodents, epididymal adipose tissue dominates in comparison with visceral adipose tissue of other localizations [34]. This correlates well with the data we obtained: in rats on a standard diet, the specific mass of epididymal adipose tissue prevailed. A high-fat diet increased the specific weight of subcutaneous and retroperitoneal adipose tissue, which in turn increased the amount of fat depots. It is known that the subcutaneous fat depot acts as one of the main reservoirs of fat accumulation and can be a protective mechanism of other tissues against lipotoxicity [35].
Visceral adipose tissue in rodents is represented by mesenteric (the structures mentioned are found intraperitoneally (along the colon), retroperitoneally (behind the kidneys), and epididymally (behind the testes) [33]. Fat depots are morphologically and biochemically different. Mesenteric adipose tissue is the most metabolically active: It is distinguished by a high degree of lipid mobility, a dense vascular network, and a vigorous blood flow, and small adipocytes predominate. Epididymal adipose tissue has a less intensive metabolism of glucose and lipids, the presence of big adipocytes is the prevailing characteristic. Retroperitoneal adipose tissue consists of adipocytes of medium and big sizes. Subcutaneous adipose tissue (subcutaneous depot of the inguinal region) has a low intensity of glucose and lipid metabolism and small adipocytes.
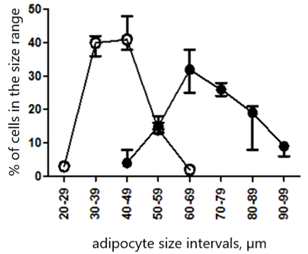
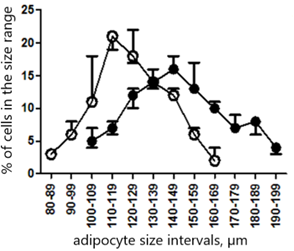
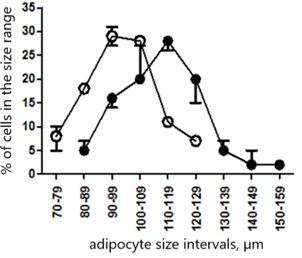
The size of adipocytes determines the metabolic activity of adipose tissue [36]. Adipocytes are heterogeneous in size within a single fat depot and can be divided into small (diameter up to 50 µm), medium (diameter from 50 to 100 µm), and large (diameter over 100 µm) [37]. The average size of mesenteric adipocytes in the group of animals on a high—fat diet was 63% larger (p<0.005), epididymal by 19% (p<0.01), retroperitoneal by 14% (p<0.01) and subcutaneous by 13% (p<0.05) compared with a group of rats receiving a standard diet (Table 2).
Table 2. The average size of adipocytes of mesenteric, epididymal, retroperitoneal, and subcutaneous adipose tissue of rats with a standard and high-fat diet, Me (Q1- Q3)
|
Me indicators (Q ₁–Q₃) |
Experimental groups |
|
|
Group 1 (control) (n=10) |
Group 2 (experienced) (n=10) |
|
|
Average size of adipocytes MAT, µm |
41.8 (36.7–48.7) |
68.8 (60.6–77.9)* |
|
Average size of adipocytes EAT, µm |
122.6 (111.3–135.5) |
146.5 (130.2–162.3)** |
|
Average size of adipocytes RAT, µm |
97.8 (89.3–106.4) |
111.9 (102.4–122.7)** |
|
Average size of adipocytes SAT, µm |
47.7 (43.2–54.4) |
54.2 (48.4–61.5)* |
Note: n is the number of animals in the group; * – p₂₋₁<0.005; ** – p₂₋₁<0.01
The change in the average size of adipocytes can be caused by two processes: hypertrophy and cell hyperplasia [38].
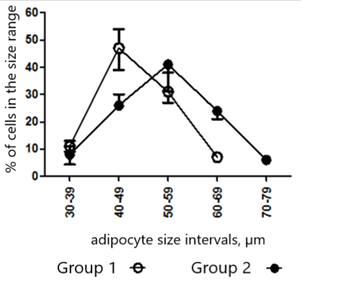
Among rats receiving regular nutrition, mesenteric adipose tissue was predominantly composed of small cells measuring up to 50 µm. In contrast, epididymal tissue consisted mainly of giant cells exceeding 100 µm in size. Retroperitoneal tissue had predominantly cells ranging from 50 to 100 µm in size. Subcutaneous tissue exhibited a mixture of both small and large cells. A high-fat diet led to the predominance of large cells (50-100 µm) in mesenteric adipose tissue, large cells (more than 100 µm) in epididymal and retroperitoneal adipose tissue, and small and large cells in subcutaneous adipose tissue (Figure 1).
|
|
|
|
a) |
b) |
|
|
|
|
c) |
d) |
|
Figure 1. Distribution of adipocytes of rat adipose tissue by size: group 1 (control) (n=10); group 2 (experimental) (n=10): a) mesenteric adipose tissue, b) epididymal adipose tissue, c) retroperitoneal adipose tissue, d) subcutaneous adipose tissue |
|
Thus, the increase in the specific mass of visceral fat depots with a high-fat diet is due to hypertrophy of fat cells, and subcutaneous adipose tissue - possibly due to hyperplasia. The change in adipose tissue mass in rats with age occurs mainly due to hypertrophy of mesenteric and epididymal adipose tissue cells, while retroperitoneal and subcutaneous adipose tissue is due to hyperplasia.
An increase in cell size of more than 80-100 µm leads to a decrease in glucose uptake, triacylglycerols, and insulin sensitivity [39]. It is known that hypertrophied cells are the main source of proinflammatory cytokines and have a limited ability to synthesize adiponectin, which is a powerful anti-inflammatory adipokine and an endogenous insulin sensitizer [40]. In hypertrophied adipose tissue, blood flow decreases, initiating local hypoxia, and infiltration by macrophages, whose cytokines inhibit adipogenesis, increases [41].
The relatively smaller rise in the average size of adipocytes in subcutaneous adipose tissue in animals on a high-fat diet, compared to the adipose tissue in visceral depots, is because there are more tiny cells present.
Therefore, the rise in subcutaneous adipose tissue mass resulting from a high-fat diet is attributed to an augmentation in smaller cells. Recent studies suggest that these cells serve to safeguard muscles and the liver against fat buildup and inhibit the onset of insulin resistance.
Conclusion
In rats on a standard diet, the specific gravity and average size of adipocytes of epididymal adipose tissue predominate. A diet rich in fat causes an elevation in the density of several forms of adipose tissue, primarily subcutaneous. The prevalence of big adipocytes is linked to an increase in the specific mass of visceral fat depots. In rats fed a high-fat diet, the subcutaneous adipose tissue is characterized by a higher proportion of tiny adipocytes compared to adipose tissue in other areas of the body.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: The protocol for experiments with laboratory animals complied with the requirements of the European Convention for the Protection of Vertebrate Animals used for Experimental and other Scientific Purposes.