Pharmacophore an International Research Journal
Momordica charantia (MC), commonly known as bitter melon, has garnered attention for its diverse pharmacological properties, particularly its potential in managing diabetes mellitus (DM) and associated complications. The present narrative review comprehensively assesses the scientific landscape surrounding MC's efficacy and safety in the context of diabetes and its related complications, encompassing neuropathy, nephropathy, impaired wound healing, retinopathy, dyslipidemia, fatty liver disease, hypertension, and atherosclerosis. Drawing insights from both experimental studies on animal models and clinical trials, the present evaluation reveals that MC exhibits notable hypoglycemic effects attributed to its rich phytochemistry, including bioactive components such as charatin, vicine, and various momordin compounds. Moreover, the herb demonstrates antioxidant, anti-inflammatory, and immunomodulatory properties, offering potential benefits in mitigating complications associated with DM. However, while animal model studies showcase promising results, clinical evidence remains somewhat inconclusive, necessitating further rigorous investigation. Nevertheless, in the context of diabetes’s incurable nature, MC emerges as a promising supplementary approach for diabetes management, showcasing mild outcomes with sustained efficacy and exhibiting a favorable safety profile.
Introduction
Hyperglycemia caused by abnormalities in insulin secretion, action, or both characterize diabetes mellitus (DM), which is considered as being the fifth greatest cause of mortality worldwide. DM is the major cause of gastrointestinal, renal, and neurological symptoms worldwide and is characterized by abnormalities in protein, lipid, and carbohydrate metabolism [1].
Medications used to treat type 2 diabetes (T2D) include insulin and anti-hyperglycemic medications such as thiazolidinediones, biguanides, sulphonylurea derivatives, dipeptidyl peptidase 4 inhibitors, sodium-glucose cotransporter inhibitors, and glucagon-like peptide 1 agonists [2].
Existing synthetic medications for diabetes exhibit drawbacks, including variations in individual responses, challenges in achieving glycemic control, and the occurrence of adverse effects. It is imperative to investigate more efficacious therapeutic approaches for individuals with diabetes. Pharmacogenomic studies of current antidiabetic agents and potential new drug targets for precision medicine for diabetes [3].
A more novel approach for treating type 2 diabetes involves the utilization of herbal treatments, which demonstrate moderate efficacy with sustained effects and a reduced incidence of adverse effects [4].
Therapies utilizing compounds derived from naturally growing plants symbolize the remarkable interactions within the body. Furthermore, herbal remedies trace their origins across diverse cultures worldwide, since ancient times [5, 6]. Herbal medicines, incorporating plant-derived compounds [7-10], are widely acknowledged for their efficacy in addressing various diseases [11-13], offering valuable remedies with minimal risk of adverse effects.
Traditional medicine practitioners in different countries have long relied on Momordica charantia (MC) to treat high blood sugar and prevent diabetes in its early stages [14]. MC, a recognized botanical specimen, is classified under the Cucurbitaceae botanical family [15]. It is widely recognized by several vernacular names, such as bitter melon, balsam pear, bitter gourd, karela, or kugua [16]. The unique flavor and nutritional profile make it a popular vegetable in many tropical and subtropical parts of the world. MC green fruits are a good source of minerals, vitamins A and C, as well as niacin, thiamine, and riboflavin [17]. Moreover, it contains a large quantity of phenolic compounds (alkaloids, gallic acid, flavonoids, saponins, etc.) [18].
The strongest antioxidant activity among the family is exhibited by MC, which is attributed to its rich phytochemistry. MC has bioactive components that give it pharmacological effects and therapeutic benefits, including hypolipidemic and hypoglycemic effects, antioxidant scavenging, and more [19, 20].
Research on the therapeutic effects of MC has revealed a wide range of properties, including anti-tumor, anti-bacterial, anti-viral, anthelmintic, antilipolytic, hypoglycemic, anti-diabetic, antioxidant, anti-inflammatory, immunomodulatory, antimutagenic, antifertility, hepatoprotective, as well as anti-ulcerogenic abilities [21].
Numerous hypotheses about the plant's anti-diabetic effects have been suggested based on extensive research in animal models. The MC seeds, stems, leaves, endosperm, pericarps, fruit, callus tissues, and cotyledons have yielded around 228 distinct chemicals that may have therapeutic effects either singly or in combination. Charatin, vicine, polypeptide-p, momordin, and related compounds (e.g., momordicin, momordicilin, momordinol, and momorcharin) are among the most researched components that have been found to enhance glycemic control [22, 23].
It is assumed that the hypoglycemic effects of MC and its constituents are expressed via a variety of biochemical, physiological, and pharmacological pathways. There are various ways in which MC and its compounds can lower BGLs; these include preserving the functions of islet β cells, blocking the uptake of Glu in the intestines, suppressing enzymes that are important for gluconeogenesis, stimulating an enzyme that is important for the hexose monophosphate pathway, stimulating the use of Glu by skeletal and peripheral muscles, and preventing the differentiation of adipocytes [24, 25].
By suppressing nuclear factor kappa B (NF-κβ) and mitogen‑activated protein kinase in pancreatic cells, MC promotes glucose (Glu) and fatty acid catabolism, induces insulin production, stimulates fatty acid absorption, activates the AMP-activated protein kinase (AMPK) pathway, ameliorates insulin resistance, and inhibits Glu metabolism enzymes (glucose-6-phosphatase and fructose-1,6-bisphosphate), thus MC shows its anti-diabetic effects [26, 27].
MC’s impressive hypoglycemic qualities make it a promising candidate as a medicinal food ingredient for the treatment of diabetes and pre-diabetes, as well as for weight management and lipid metabolism regulation [28].
The present narrative review aims to provide a comprehensive evaluation of MC in the context of diabetes mellitus. Drawing insights from in vitro models, animal model experimental studies, and clinical trials, the objective is to highlight the current state of knowledge regarding MC's efficacy and safety profile. Through a comprehensive examination of the data, we aim to offer a scientifically informed perspective on MC's therapeutic implications for diabetes, facilitating a nuanced understanding that may guide further research and clinical exploration.
Materials and Methods
The present narrative review screens, filters, and evaluates scientific publications highlighting the influence of MC phytocompounds in the regulation of pathophysiological processes occurring in DM and related pathologies, providing the current state of knowledge in this phytotherapeutic subfield by comprehensively characterizing the link between bioactive compounds and therapeutic activity, the antidiabetic activity observed in cell culture studies, animal models, and especially clinical studies, as well as presenting a detailed safety and efficacy profile of MC.
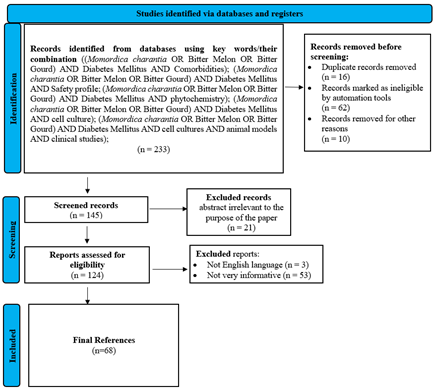
In order to achieve this goal, an algorithm was established using Boolean operators and allowing a detailed search in some of the databases with wide coverage in the medical field. Figure 1 shows the procedural framework regarding the steps of selection of publications for final inclusion in the list used as bibliographic references for this paper. This process was based on the recommendations provided by Page et al. [29].
|
|
|
Figure 1. The algorithm for evaluating the selection of bibliographic sources. |
Non-English publications or those lacking relevance to the current paper, as well as those not adhering to the article or book format, were omitted. A comprehensive selection procedure resulted in 68 bibliographic references spanning from 1990 to 2023, cited for data validation in this study. Moreover, in order to have a clear view of the research areas for the topic evaluated in the present manuscript, Figure 2 illustrates the primary ten Web of Science categories (displayed using the search terms ‘Momordica charantia and Diabetes Mellitus’) with the highest manuscript distribution. Scientific journal publications are categorized within relevant classifications, and each journal in the Web of Science database receives one or more assigned classifications. Most of the papers were allocated to the "Pharmacology Pharmacy" category, with "Integrative Complementary Medicine" ranking second in distribution.
|
|
|
Figure 2. The top ten research areas in the Web of Science Core Collection for the algorithm used. |
Bioactive Compound's Therapeutic Activity Relationship
Researchers worldwide have extracted approximately 228 distinct medicinal compounds from various parts of MC, including stems, leaves, pericarp, the entire plant, aerial parts, endosperm, callus tissues, cotyledons, seeds, and unripe fruit [30].
MC was used to isolate functional polysaccharides. The branched heteropolysaccharide bioactive polysaccharide from MC (MCBP) had a molecular weight of 92 kDa and was acidic. According to the results of the Fourier transforms infrared spectroscopy, MCBP is a pectin-like polysaccharide that contains many monosaccharides, the most common of which are galactose (Gal), Glu, and galacturonic acid, and it has an esterification degree of 53%. The results also demonstrated that MCBP had ferric-reducing antioxidant power (0.95 mM), the ability to scavenge free radicals, inhibit α-amylase, and angiotensin-converting enzyme [31].
MC lectin, ribosome-inactivating proteins, Momordica anti-HIV protein of 30 kDa, α-, β-, γ-, δ- and ε-momorcharin, and several others, have been isolated from various parts of MC. These proteins and peptides have been shown to exhibit polynucleotide adenosine glycosidase activity, RNA N-glycosidase action, DNase-like activity, superoxide dismutase activity, phospholipase activity, anti-cancer, anti-tumor, antimicrobial and immunosuppressive properties [32].
Various extraction methods have been used to separate crude polysaccharides from MC (MCP), including the more conventional hot-water, alkali, and acid extractions, as well as extractions assisted by microwave, enzymes, and ultrasonic, followed by ethanol precipitation. Glu, Gal, rhamnose (Rha), arabinose (Ara), and mannose are the polysaccharides that comprise around 6% of MC powder. These polysaccharides are referred to as heteropolysaccharides [33].
Using ion exchange and size-exclusion chromatography, a polysaccharide having a molecular weight of 13,029 Da was extracted from the fruit of MC. The MCPIIa, the polysaccharide that was extracted comprised D-Gal, D-GalA, D-Xyl, L-Ara, and L-Rha. A multitude of glucuronic acid, arabino furanose, and xylopyranosyl residues were connected to the MCPIIa sugar units through β-glycosidic bonds, as revealed by nuclear magnetic resonance investigations and infra-red (IR) spectra [34].
The investigation into the phytochemical composition of MC fruits led to the identification of two novel (1 and 2) and eight known cucurbitane-type triterpene glycosides, along with one cucurbitane-type triterpene. The glycosides (1 and 2, momordicosides A, F (1), F (2), G, K, and L, goyaglycoside-c, and goyaglycoside-d) and the triterpene [3 beta,7 beta,25-trihydroxycucurbita-5,23(E)-dien-19-al] were characterized through various analytical techniques [35].
The Cucurbitaceae family is a rich source of saponins with diverse biological effects. Saponins from MC were extracted using high hydrostatic pressure (HHP) technology. Liquid chromatography-mass spectrometry assessment identified four saponins, including kuguaglycoside A, momordicoside L, kuguacin B, and kuguacin J, laying the groundwork for exploring their biological activity [36].
Charantin, a representative cucurbitane-type triterpenoid found in MC, possesses promising attributes as a substance with potential antidiabetic properties [25]. In laboratory and clinical settings, researchers have conducted in vitro and in vivo studies using a variety of water, ethanol, and ether extracts in order to explore the hypoglycemic effects of isolated biologically active phytochemicals, such as glycosides (e.g., momordin and charantin), alkaloids (e.g., momordicin), polypeptide-P, seed oils containing linoleic, stearic, and oleic acids, and glycoproteins like alpha–momorcharin, beta-momorcharin, lecithins, protein MAP30, and vicine [37, 38]. Furthermore, Polypeptide-P, a glycoprotein peptide, exhibits hypoglycemic properties [39] and is sourced from the fruit, seeds, and tissues of MC [40-42].
Five new cucurbitane-type triterpene glycosides compounds (e.g., charantosides K (3), J (2), goyaglycoside-l (5), charantosides H (1), and momorcharacoside A (4)) were isolated from the ethanolic extract of MC fruits. All compounds were tested for their inhibition against α-glucosidase, revealing that compounds 2 and 5 displayed moderate inhibitory activities as compared to the positive control [43].
An experimental investigation was conducted to compare the antiglycation and antioxidant properties of aqueous extracts of MC pulp, MC flesh, and charantin in vitro. Additionally, the phenolic, flavonol, and flavonoid contents of the extracts were determined. The results indicated that all extracts exhibited a dose-dependent inhibition of the formation of crosslinked advanced glycation end-products and carboxymethyllysine, with MC flesh being identified as the most potent among them [44].
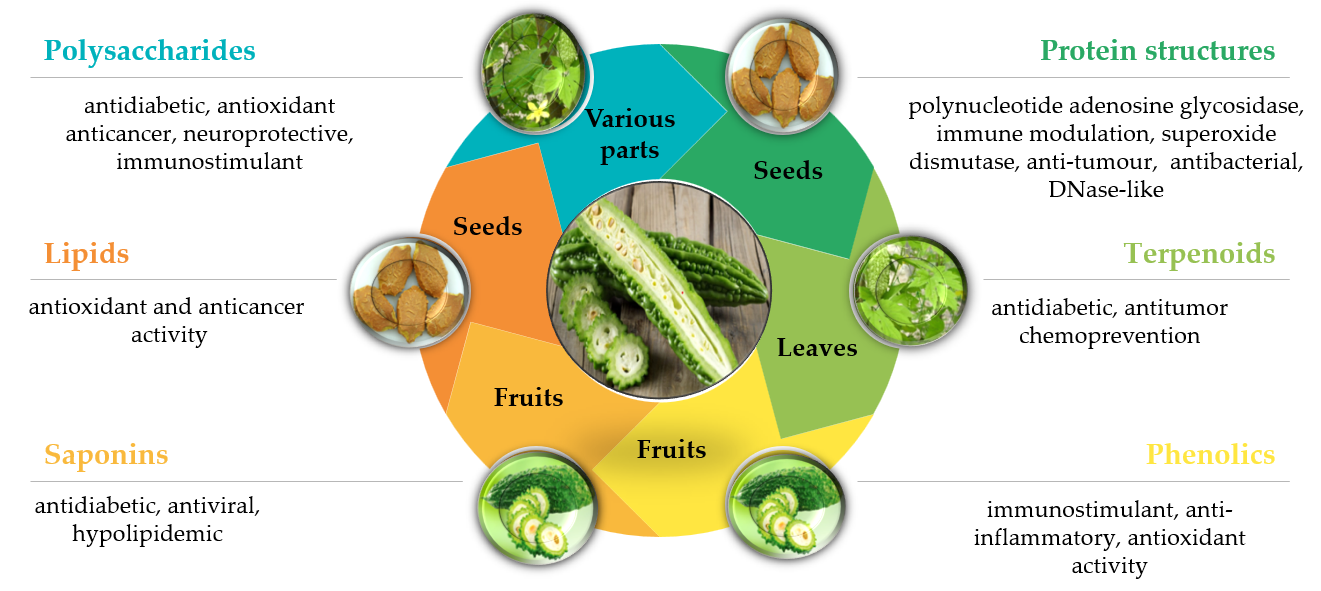
In another experimental study, MCP was extracted using hot water and subsequently subjected to chemical modification. This modification process resulted in the production of sulfated MC polysaccharide (S-MCP) with a degree of substitution of 0.45 and phosphorylated MC polysaccharide (P-MCP) with a degree of substitution of 0.12. The three polysaccharides had the sugar contents measured by the phenol sulfuric acid method (74.0%, 59.8%, and 68.1%). It was found the degree to which the three different polysaccharides reduced and prevented lipid peroxidation, in addition to how well they scavenged hydroxyl radical, superoxide anion, and DPPH radicals. The results of the mentioned research demonstrated that various chemical changes of polysaccharides resulted in varying degrees of antioxidant activity [45]. Figure 3 illustrates the correlation between the major bioactive components, their pharmacological activity, and their distribution in the different parts of MC [41]. When given subcutaneously to humans, gerbils, and langurs, polypeptide-p, which was isolated from MC seeds and fruits, displayed effective hypoglycemic effects [46]. Some of the many favorable physiologic effects shown by momordicosides (Q, R, S, T, and U) and karaviloside XI on diabetes include promoting the oxidation of fatty acids, increasing the entrance of inducible Glu into cells, and facilitating the disposal of Glu [47].
A promising compound charantin, found in medicinal plants like MC, is a triterpenoid of the cucurbitane class that may have antidiabetic effects [25].
|
|
|
Figure 3. Bioactive components, pharmacological activity, and distribution across various parts of MC. |
Antidiabetic Benefits Demonstrated in Scientific Studies
Experimental Studies On Cell Culture Models
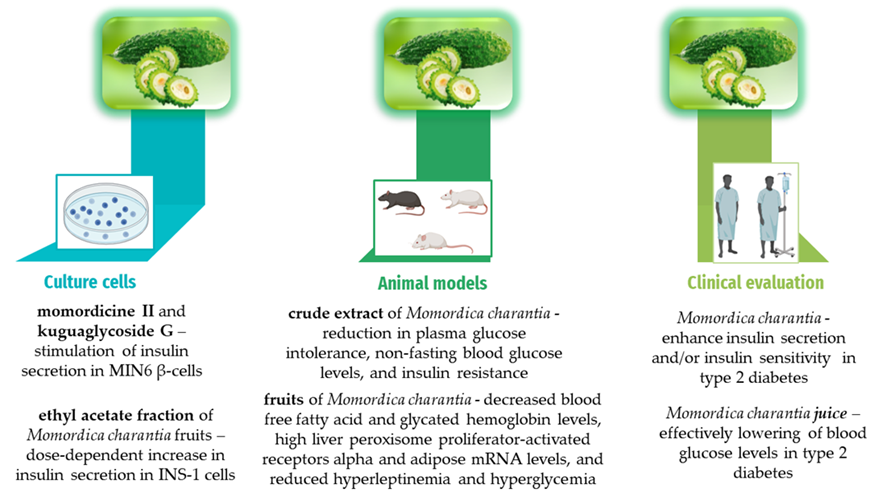
Some saponins isolated from MC may exhibit antidiabetic activity. An experimental study investigated the impact on insulin secretion using MIN6 β-cells exposed to an ethanol extract, a saponin-rich fraction, and five purified saponins and triterpenoids from MC: 3β,7β,25-trihydroxycucurbita-5,23(E)-dien-19-al (the first compound), momordicine I (the second compound), momordicine II (the third compound), 3-hydroxycucurbita-5,24-dien-19-al-7,23-di-O-β-glucopyranoside (the fourth compound), and kuguaglycoside G (the fifth compound). All five compounds were compared to high glucose and the insulin secretagogue glipizide. Results showed that at 125 μg/mL, a saponin-rich fraction significantly enhanced insulin secretion compared to the dimethyl sulfoxide vehicle. Compounds three and five, at concentrations of 10 and 25 μg/mL, respectively, also significantly stimulated insulin secretion compared to the vehicle. The study marked the first instance of a saponin-rich fraction and isolated compounds, particularly three and five, from MC exhibiting insulin-stimulating effects in an in vitro static incubation assay [48].
In another experimental study, the investigation focused on the influence of MC fruit on insulin secretion from β-cells and the underlying mechanisms. The green fruit underwent a freeze-drying process and subsequent extraction with methanol. The resulting MC fruit extract was subjected to fractionation into ethyl acetate (fraction A), n-butanol (fraction B), and water (fraction C). The assessment of insulin secretory capacity involved the utilization of the extract and its fractions on INS-1 rat insulinoma cells, rat pancreatic islets, and the execution of an oral glucose tolerance test on rats. Simultaneously, an examination of adenosine triphosphate production in β-cells was conducted. The extract demonstrated a dose-dependent increase in insulin secretion from INS-1 cells, irrespective of glucose dosage. Significantly, fraction A (the hydrophobic fraction) exhibited an augmentation in insulin secretion comparable to that observed with the extract, while fractions B and C displayed no such effect. This observed outcome remained consistent in pancreatic islets as well [49].
Experimental Studies on Animal Models
Moreover, streptozotocin (STZ)-induced diabetic mice were used to study the hypoglycemic effect of MCPIIa. The STZ-induction was followed by 28 days of oral administration of MCPIIa at doses of 100, 200, or 300 mg/kg body weight. After receiving MCPIIa, STZ-diabetogenic mice showed a considerable improvement in their glycemia and a marked increase in blood insulin concentration compared to DM mice. Mice given MCPIIa had fewer STZ-lesions in their pancreatic tissue, as shown by transmission electron microscopy. These findings suggest that MCPIIa may be a potential diabetes treatment [34].
The hypothesis that MCP has a reno-protective effect by assessing the antioxidant capacity, oxidative stress markers, anti-lipidemic and anti-hyperglycemic effects in diabetic rats induced with STZ was investigated in a different study. The value of kidney function tests in the rats that had been diabetic due to STZ was significantly normalized after oral administration of MCP. When comparing normal rats with STZ-induced diabetic rats, the concentrations of blood urea nitrogen (BUN), creatinine, and urea protein, were found to be 316.58%, 800.97%, and 195.14% higher, respectively. In addition to a marked decrease in MDA, glutathione peroxidase (GPx), superoxide dismutase, and catalase (CAT) levels all showed substantial improvements after MCP treatment for diabetic kidneys [50].
The following presented study aimed to examine the variances in the anti-diabetic characteristics and mechanism of action of Taiwanese MC in mice with T1D and T2D. In order to elucidate the advantageous impacts of MC, oral glucose tolerance test (OGTT), non-fasting Glu, and plasma insulin levels in KK/HIJ mice with high-fat diet (HFD) -induced diabetes and treated with a dosage of 200 mg/kg/day of charantin-rich extract of MC (CEMC) were conducted. Additionally, were performed the same measurements in ICR mice that had STZ-induced diabetes. Following 8 weeks, the mice were subjected to exsanguination, and subsequently, the expression of insulin-signaling-associated proteins from their tissue was assessed. This evaluation was conducted in conjunction with an examination of the protective actions of CEMC against pancreatic β-cell toxicity in an in vitro setting. The results collected over eight weeks demonstrated that the administration of CEMC resulted in a notable reduction in plasma Glu intolerance, non-fasting BGLs, and insulin resistance specifically in the KK/HIJ mice. However, no significant effects were observed in the ICR mice [51].
The initial phase of another study was centered on the identification of primary bioactive constituents, namely vicine and charantin, in various segments of the fruit of the plant under investigation. During the second part of the study, Sprague Dawley rats with hyperglycemic and normal conditions were administered MC in the form of entire fruit, skin, or flesh. The dosage levels used were 150 and 300 mg/kg body weight. The rats were then evaluated to determine the effectiveness of MC in preventing and treating diabetes. The entire fruit contained the most vicine while fruit flesh contained the most charantin. When given to healthy rats, MC helped slow the development of diabetes. Diabetic complications such as polyuria, increased glomerular filtration rate, renal hypertrophy, glycosuria, and polydipsia were observed in hyperglycemic rats. On the other hand, these metrics improved significantly after MC consumption [52].
Researchers looked at the effects of MC juice on rats with DM caused by STZ and how it functions. BGLs, systolic blood pressure (SBP), and osmolarity, significantly increased throughout the disease, while insulin-positive cells per islet and body weight significantly decreased throughout the disease, in comparison to healthy controls of the same age. Ingesting MC juice orally partially counteracted all of the diabetes-related symptoms observed in rats with diabetes induced with STZ. The sugar absorption by the jejunum's brush border membrane vesicles, which is dependent on Na+ and K+, was considerably reduced in STZ-induced diabetic rats after daily oral treatment with MC juice, in comparison to responses seen in STZ-induced diabetic rats. One way to accelerate 14C-D-glucose uptake in L6 myotubes is with insulin (100 MM), while another is with the lyophilized extract of fruit juice (5 microg x mL(-1)). Wortmannin, a phosphatidylinositol 3-kinase inhibitor, entirely suppressed these effects [48].
Investigators looked at how MC fruits affected hyperglycemia and insulin resistance in C57BL/6J mice that were given an HFD. Starting with 12 weeks of 45% HFD, the experimental group of mice was then randomly assigned to a different group from the control group, which received a low-fat (LF) diet. Eight weeks into the induction period, the high-fat (HF) group was further divided into six equal parts and given oral doses of rosiglitazone or MC four weeks subsequently. Researchers found that MC decreased blood free fatty acid (FFA) and HbA1c levels, high liver peroxisome proliferator-activated receptors (PPAR) alpha and adipose PPAR gamma mRNA levels, and reduced hyperleptinemia and hyperglycemia generated by the HFD. Adipose resistin and leptin mRNA levels were also reduced, and the weights of visceral fat and epididymal white adipose tissue were considerably reduced, after consuming MC. One possible explanation for MC effects is that it modulates insulin resistance and Glu levels via PPAR gamma-mediated pathways, while another possible explanation is that it modulates plasma lipid profiles through PPARalpha-mediated pathways [49].
The effects of MC, on rats with T2D produced by STZ were examined in another investigation. in which researchers divided the male Wister rats into four groups at random. Oral administration of MC fruit juice (10 mL/kg/day) was performed on diabetic rats in three groups: Group I, the normal control group; Group II, the STZ diabetic group; and Groups III and IV, the diabetic rats treated with the juice for 21 days after diabetes induction, or as a prophylactic measure for 14 days before induction. Isolated diaphragm muscles from rats were tested for Glu absorption with and without insulin to determine the in vivo and in vitro effects of MC juice. Additionally, the pancreas was the histopathologic point of view. Results demonstrated that MC significantly decreased total cholesterol, insulin resistance index, pancreatic malondialdehyde (MDA) content, fructosamine, triglycerides, and BGLs in both prevention and therapy. Although it ameliorated histopathological alterations in the pancreas and caused a notable rise in serum insulin, β cell activity percent, total antioxidant capacity levels, HDL-cholesterol, and pancreatic reduced glutathione (GSH) content, it did not alleviate the underlying causes. Regardless of insulin presence or absence, it enhanced Glu absorption by the diaphragms of both healthy and diabetic rats [53].
In another study, the C57BL/6J mice were initially divided into two groups using a random distribution. The first group, referred to as the control (CON) group, was provided with a LF diet. On the other hand, the second group, known as the experimental group, was given an HFD consisting of 45% fat content. This dietary intervention was maintained for 8 weeks. Following that, the vehicle was administered to the CON group. In contrast, the HF group was divided into five subgroups, each of which continued to follow the HFD but received either oral rosiglitazone (Rosi) or MC extract (MCE) or no medication at all for four weeks. MC reduced Glu levels and visceral fat weights. One of the most important cellular regulators of lipid and Glu metabolism is AMPK. Phosphor pyruvate carboxykinase (PEPCK) expression is downregulated and Glu synthesis is upregulated by MCE, which raises AMPK phosphorylation in the liver by 126.2-297.3%. The 11beta-HSD1 gene, which contributes to the attenuation of the diabetic condition, had its expression reduced by MCE. This was the most noteworthy finding. Additionally, MCE reduced serum TGs by suppressing hepatic fatty acid synthesis, which was achieved via reducing fatty acid synthase mRNA and sterol response element binding protein 1c. The results show that MC improves diabetic and hyperlipidemic conditions in HF-fed mice by controlling the phosphorylation of liver 11beta-HSD1, PEPCK, and AMPK [54].
Another study set out to examine how MC extract affected insulin sensitivity and the pathways that trigger proximal insulin signaling in rats that were given an HFD. The Glu tolerance and insulin sensitivity of male Wistar rats were found to be lower after 10 weeks of HFD as compared to rats that were fed chow. Glu tolerance and sensitivity to insulin were enhanced by supplementing with MC extract for two weeks during the ninth and tenth weeks of HFD. Furthermore, the HFD elevated fasting insulin, cholesterol, and epididymal fat; however, MC extract decreased the levels of these parameters. Insulin-stimulated insulin receptor tyrosine phosphorylation, insulin receptor substrate-1 (IRS-1), and skeletal muscle insulin receptor were unaffected by MC supplementation and high-fat diet in comparison to rats fed chow. In contrast to control rats, rats given a high-fat diet for 10 weeks had less insulin-stimulated IRS-1 tyrosine phosphorylation. The addition of MC supplementation, combined with an HFD, for two weeks, resulted in an enhancement of insulin-stimulated IRS-1 tyrosine phosphorylation as compared to rats just fed with the HFD. The findings of the study indicate that the administration of MC extract has a positive impact on insulin sensitivity, Glu tolerance, and insulin signaling in a model of insulin resistance generated by a high-fat diet [55].
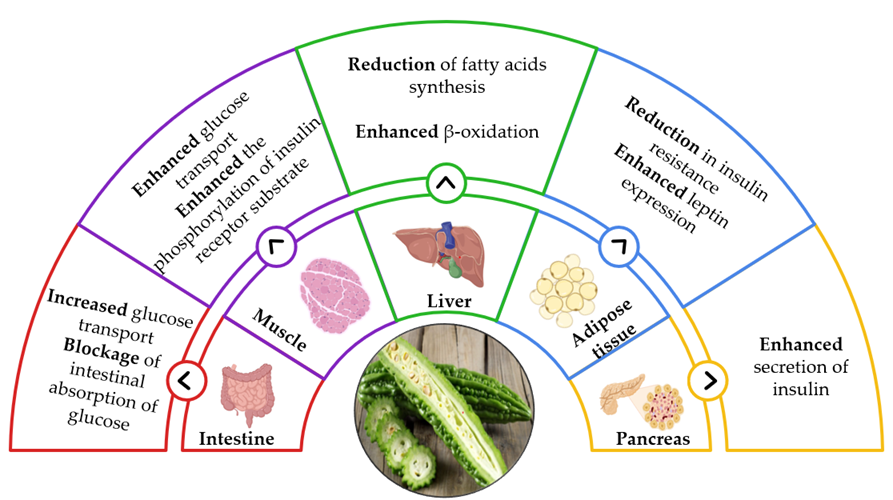
Figure 4 illustrates some of the most important mechanisms through which MC modulates biochemical parameters, thereby contributing to the amelioration of diabetes management and the reduction of associated risks [15, 56].
|
|
|
Figure 4. Mechanisms underlying the antidiabetic action of MC. |
Clinical Evaluations
Traditional functional foods and medicines made from MC are popular in Asia. In individuals diagnosed with type I diabetes (T1D) or T2D, the 166 AA polypeptide known as Polypeptide-P has been found to exhibit hypoglycemic effects. This peptide gene sequence is yet unknown; however, its AA sequence has been identified. Using degenerate reverse transcription polymer chain reaction and genome-walking, this study employed a gene-cloning procedure to get the polypeptide-P gene sequence. The polypeptide-P protein's whole 498 base pair sequence has been recreated from MC seeds. Bioactivity tests conducted on the generated recombinant protein later showed that it significantly reduced BGLs in mice with diabetes caused by alloxan. This finding provides more evidence that recombinant polypeptide-P can lower BGLs [39].
The objective of another research was to determine whether an MC peptide with a specific 19-amino acid (AA) sequence (mcIRBP-19) might effectively control BGLs in individuals with diabetes. A total of 142 individuals with diabetes were included in the trial; 78 were assigned to a control group and 64 were distributed to an experimental group so that the product could be tested with the particularly processed MC peptide. A paired t-test was used to compare biochemical data and confirm the statistical significance of variations during different time intervals. According to the clinical outcomes, the individuals' glycated hemoglobin (HbA1c) concentrations began to improve by the end of the second month (T2) after receiving the MC peptide. The mean values of these improvements were considerably smaller. The results dropped steadily until they were 7.4 ± 1.1% at the end of the study (T3). During the same interval, there was no significant difference in the control group's HbA1c values, which were 7.5 ± 1.2% in T0 and 7.5 ± 1.1% in T3. The results of the clinical trial lend reliability to the idea that the novel MC peptide medication successfully controls BGLs in diabetics [57].
Researchers suggested that, in the absence of pharmaceutical intervention, MC supplementation would enhance insulin secretion and/or insulin sensitivity in type 2 diabetic patients. The investigators wanted to see how taking MC affected insulin secretion and sensitivity. For three months, 24 patients participated in a randomized, double-blind, placebo-controlled clinical trial where they were given either 2000 mg of MC daily or a placebo. Before and after the intervention, participants underwent a 2-hour OGTT to determine insulin sensitivity (Matsuda index), the area under the curve (AUC) for Glu and insulin, total insulin secretion (insulinogenic index), and the initial phase of insulin secretion (Stumvoll index). Subjects treated with MC showed statistically significant reductions in several measures of metabolic health, HBA1c, 2-h Glu in OGTT, including weight, waist circumference (WC), fat percentage, BMI, and AUC of glucose. Insulin AUC, and the first phase of insulin secretion and total insulin secretion, were all significantly increased following MC administration. The results showed that the treatment with MC resulted in a decrease in Glu AUC, HBA1c, 2-h Glu, fat percentage, BMI, weight, and WC, along with an increase in insulin AUC, total and first-phase insulin secretion [58].
Participants in an OGTT were ten adults at risk of developing diabetes, they took Glu alone (D2), and MC with Glu (D3). Subjects were considered to be responders if their AUCglu during D3 was less than D2 during D2. Participants were divided into two groups based on their Glu response pattern: Slowpeak (Glupeak after 30P) and Fastpeak (peak Glu, or Glupeak, at 30 minutes post-Glu, or 30P). This allowed us to assess the immediate effects of the beverage across individuals with different levels of Glu tolerance. D3 showed a decrease of 13.2% in AUCglu, 10.6% in Glupeak, and 12.2% in mean Glu, among the responders (n=5). Plasma Glu, decreased by 9.1% at 30P, −24.0% at 60P, and −20.0% at 90P. Fastpeak and Slowpeak did not differ between trials. In half of the patients, taking MC before the third (D3) decreased their postprandial Glu, response but did not affect their insulin response. The respondents' Glu, tolerance level also did not appear to affect the beverage's efficacy. It is unclear why just some of the study's subjects had a positive reaction to the MC extract, even though MC helps diabetics maintain their BGLs [59].
In another intervention trial, prediabetic participants took 2.5 g of MC powder every day for eight weeks to see if it had any antidiabetic effects. After drinking either cucumber or MC juice, 52 people with prediabetes participated in a randomized, placebo-controlled, single-blind research experiment. A crossover design was selected with eight weeks of research time for each period and four weeks of washout in between to minimize the effect of within-subject differences in the study population. The major outcome variable that was considered was fasting plasma Glu. The CROS analysis showed a significant difference of 0.31 mmol/L in the change of FPG when comparing the various exposures. With a power of 0.82 and an effect size ranging from medium to big, the 44 final data sets were analyzed. Another model that confirmed the effect was a general linear mixed model. The impact was more noticeable with higher starting BGL, albeit not all subjects responded. There were no major side effects noted. In prediabetes, using MC supplements helped bring fasting plasma Glu levels down. The results suggest that MC may be useful for dietary self-management and Glu lowering, but additional intervention trials are needed to confirm these claims, particularly in areas without easy access to medical professionals [60].
In a trial, Indian patients with T2D (50-65 years old) were given a 7-day course of MCE (CCl4 + C6H6 MC soft extract) in addition to a half-dose oral hypoglycemic agent (glibenclamide, metformin, or a mix of the two). The results showed that the hypoglycemic effect was stronger than that of full-dose hypoglycemic drugs, suggesting that the two agents work together [61].
The following investigation compared metformin to three dosages of MC to determine their relative efficacy and safety. The trial was an active-control study that was conducted for four weeks and was randomized and double-blinded. Four groups of patients were randomly assigned to receive either 1,000 mg of metformin daily or 500 mg, 1,000 mg, or 2,000 mg of MC daily. A 4-week follow-up was conducted on all patients. By week 4, fructosamine levels had dropped significantly in both the metformin and MC 2,000 mg/day groups. There was no discernible effect of MC at doses of 500 or 1,000 mg/day on fructosamine concentrations. At a dosage of 2,000 milligrams per day, MC significantly decreased fructosamine levels from baseline and had a small hypoglycemic impact in those with T2D. On the other hand, MC had a lower hypoglycemic influence than 1,000 mg of metformin daily [62].
A different study aimed to determine whether or not MC supplements improved the glycemic and lipid profiles of patients with T2D who were already taking conventional medications. Following ethical approval, a comparative study was carried out from July 2015 to May 2016 at B P Koirala Institute of Health Sciences, Internal Medicine Department, Dharan. The study included 22 individuals with T2D who did not have any complications. For 90 days, patients in Group A received just allopathic medication (oral anti-diabetic drugs), while those in Group B received allopathic medication with 200 mL of MC juice daily. Investigators evaluated lipid profile values, fasting blood sugar, and postprandial blood sugar at baseline and 90 days after supplementation. The data was recorded in the Statistical Package for the Social Services, version 20.0, and an independent t-test was used for the statistical analysis. A combination of anti-diabetic medication and an additional 200 mL of MC per day greatly decreased fasting and postprandial blood sugar. Medications used to treat diabetes slightly lowered fasting and postprandial BGLs. Lipid profiles were improved, although not significantly, by both anti-diabetic medications individually and by MC in combination with anti-diabetic treatments When combined with allopathic medication, the juice of MC, 200 mL daily, effectively lowers BGLs in people with T2D [63].
Figure 5 shows a summary of prevalent antidiabetic effects observed in cell culture [47, 64], animal models [34, 55, 65], and clinical studies [66-68] in close correlation with the bioactive compounds contained in MC.
|
|
|
Figure 5. Results observed in different types of studies. |
Conclusion
MC emerges as a compelling candidate for the management of diabetes and its associated complications. The herb's hypoglycemic properties, coupled with its antioxidant and anti-inflammatory effects, present a multifaceted approach to addressing the complex pathophysiology of diabetes. While experimental studies on animal models offer encouraging insights, the variability in clinical outcomes underscores the need for more extensive, well-controlled human trials.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: None