Pharmacophore an International Research Journal
Obsessive-compulsive disorder (OCD) is a severe and intricate mental illness that profoundly impacts the lives of individuals affected by it. This comprehensive review aims to thoroughly explore all facets of OCD, encompassing its clinical presentations, prevalence as a common mental disorder, its neurological underpinnings, treatment modalities, and broader societal implications. The subsequent overview seeks to advance mental health awareness and foster empathy by integrating diverse perspectives and synthesizing existing research findings. Ongoing research endeavors are delving into the potential therapeutic uses of ketamine, known for its dissociative properties, as well as psychedelic substances in combination with psychotherapeutic interventions, as innovative approaches to treating OCD. Additionally, the utilization of mindfulness-based interventions, particularly mindfulness-based cognitive therapy (MBCT), is actively being investigated, along with the potential effectiveness of repetitive transcranial magnetic stimulation (rTMS) as an adjunct therapy for obsessive-compulsive disorders. The incidence of suicide attempts among individuals diagnosed with OCD varies widely, ranging from 6% to 51.7%, with an average occurrence of 14.2%. In this review, an updated elaboration of all aspects of the disorder has been given.
Introduction
Obsessive-Compulsive Disorder (OCD) profoundly impacts individuals with persistent distressing thoughts and repetitive behaviors. It's a chronic condition affecting diverse backgrounds and imposing a significant societal burden [1]. The onset of fixations frequently triggers a surge in stress and anguish, lightened by ensuing compulsions. Common fixations incorporate fears of defilement, concerns hurting oneself or others, the requirement for symmetry, devout or moralistic stresses, and meddling considerations [2]. OCD involves obsessions (unwanted thoughts) and compulsions (repeated behaviors). Common obsessions include fears of contamination, while common compulsions include cleaning and checking. OCD is categorized under obsessive-compulsive and related disorders in the DSM-5 [3-5] OCD affects 1-3% of the global population across all ages and has a lasting impact on relationships and work. Understanding genetic, neurobiological, and environmental factors is crucial for effective treatment [6]. Neurobiological studies of OCD implicate brain regions like the orbitofrontal cortex, caudate nucleus, and thalamus, elucidating neural circuit complexities. Genetic research underscores hereditary influences on susceptibility. Treatment modalities encompass Selective serotonin reuptake inhibitors (SSRIs) and Cognitive behavioral therapy (CBT), particularly Exposure and response prevention (ERP), showing promising outcomes when combined [7-9]. The present review gives a detailed account on OCD starting from its history to its treatment for the better understanding about the disease by the researchers and medical person.
Brief History
Historical records dating back centuries describe obsessions and compulsions, with accounts found in texts like the Malleus maleficarum from the 15th century. These phenomena were initially interpreted through religious lenses, as evidenced by accounts of exorcisms. However, by the 19th century, figures like Jean-Étienne Dominique Esquirol began to define obsessions and compulsions in psychiatric terms, linking them to conditions like melancholy. By the early 20th century, the understanding of OCD shifted towards psychological explanations [10, 11]. In the nineteenth century, the rise of faculty psychology, phrenology, and mesmerism influenced the understanding of neurosis as a neuropathological disorder, laying the groundwork for modern concepts of OCD. Philosophical, physiological, and political ideas shaped medical approaches to mental illness during this time. In the 1950s, learning theories extended from phobic disorders to OCD symptoms, leading to the development of behavioral therapy. While successful in reducing compulsive rituals, these theories proved insufficient to explain all OCD symptoms. By the 1980s, research focused on the relationship between OCD and neurological conditions such as epilepsy, Tourette's syndrome, and memory problems [12-14].
Prevalence and Demographics
In the US, approximately 2.3% of individuals experience OCD at some point in their lives, with prevalence rates ranging from 1% to 2.3% among children and teenagers under 18. OCD typically begins early, with an average onset age of 19.5 years [4, 15, 16]. Determining the age of onset and duration is critical in evaluating OCD, but definitions of childhood-onset versus adult-onset vary. Childhood-onset OCD may differ from adult-onset cases in characteristics and risk factors, with a higher frequency in males. The incidence of OCD has a bimodal distribution, with peaks in early childhood and early adulthood, exhibiting distinct gender distributions [17-19]. Recent research shows gender differences in OCD symptom onset: females typically experience symptoms after age 10, peaking during adolescence, while around 25% of males experience symptoms before age 10 [20].
Etiology of OCD
A complex interplay of genetic, neurological, cognitive, and environmental factors contributes to the development of OCD. Exploring these domains is crucial to understanding the diverse origins and maintenance of this mental condition
Types of OCD
Pharmacological Interventions
Treatment for obsessive-compulsive disorder (OCD) often involves pharmacological interventions focused on influencing neurotransmitter systems, particularly serotonin modulation. Medications prescribed for OCD aim to address the complex interplay of neurotransmitters, notably serotonin, to reduce symptoms and improve treatment outcomes.
Sertraline, for example, functions as a selective inhibitor of serotonin reuptake, prolonging serotonin transmission. Its long elimination half-life of approximately 26 hours allows for once-daily dosing, making it convenient for OCD treatment [39].
Sertraline strongly inhibits serotonin uptake, with minimal impact on dopamine and noradrenaline. It reduces serotonin turnover acutely and prevents depletion of central serotonin stores. It down-regulates central β-adrenoceptors and lacks significant affinity for muscarinic and histamine receptors. Sertraline is slowly absorbed orally, peaking 4 to 8 hours post a 100mg dose. It has linear pharmacokinetics within a 50 to 200mg dosage range, with increased bioavailability and peak plasma concentrations in the presence of food. It is extensively distributed in tissues, metabolized in the liver, and has a 26-hour elimination half-life, supporting once-daily dosing [39].
|
|
|
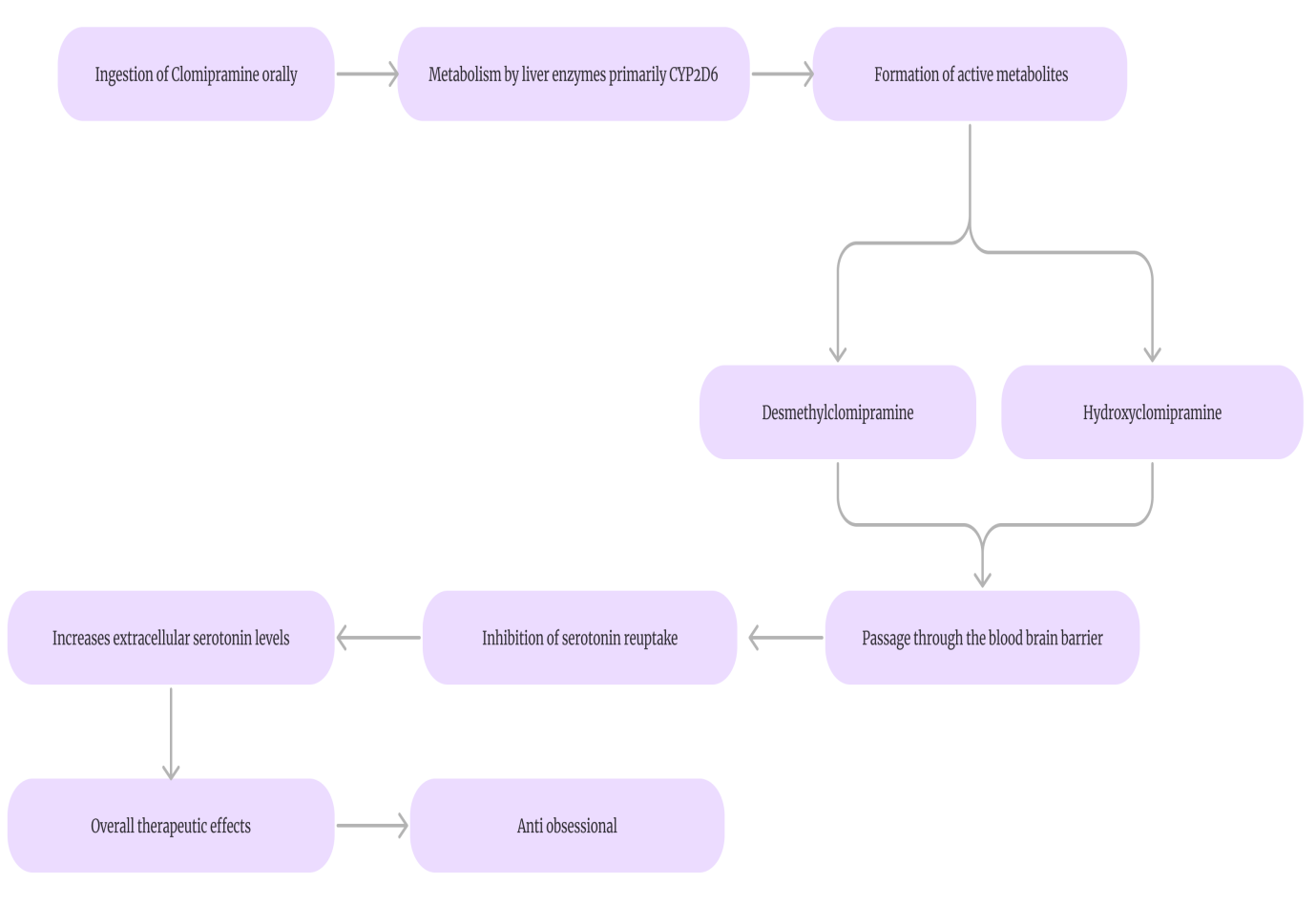
Figure 1. Mechanism of action of clomipramine |
Clomipramine is a drug taken orally to treat OCD, and it is primarily metabolized by the liver through CYP2D6. Metabolites such as desmethylclomipramine and hydroxyclomipramine raise serotonin levels outside cells by blocking reuptake, aiding in the effectiveness of treatment. These activities take place past the blood-brain barrier, boosting serotonin functions important for controlling symptoms of OCD.
|
|
|
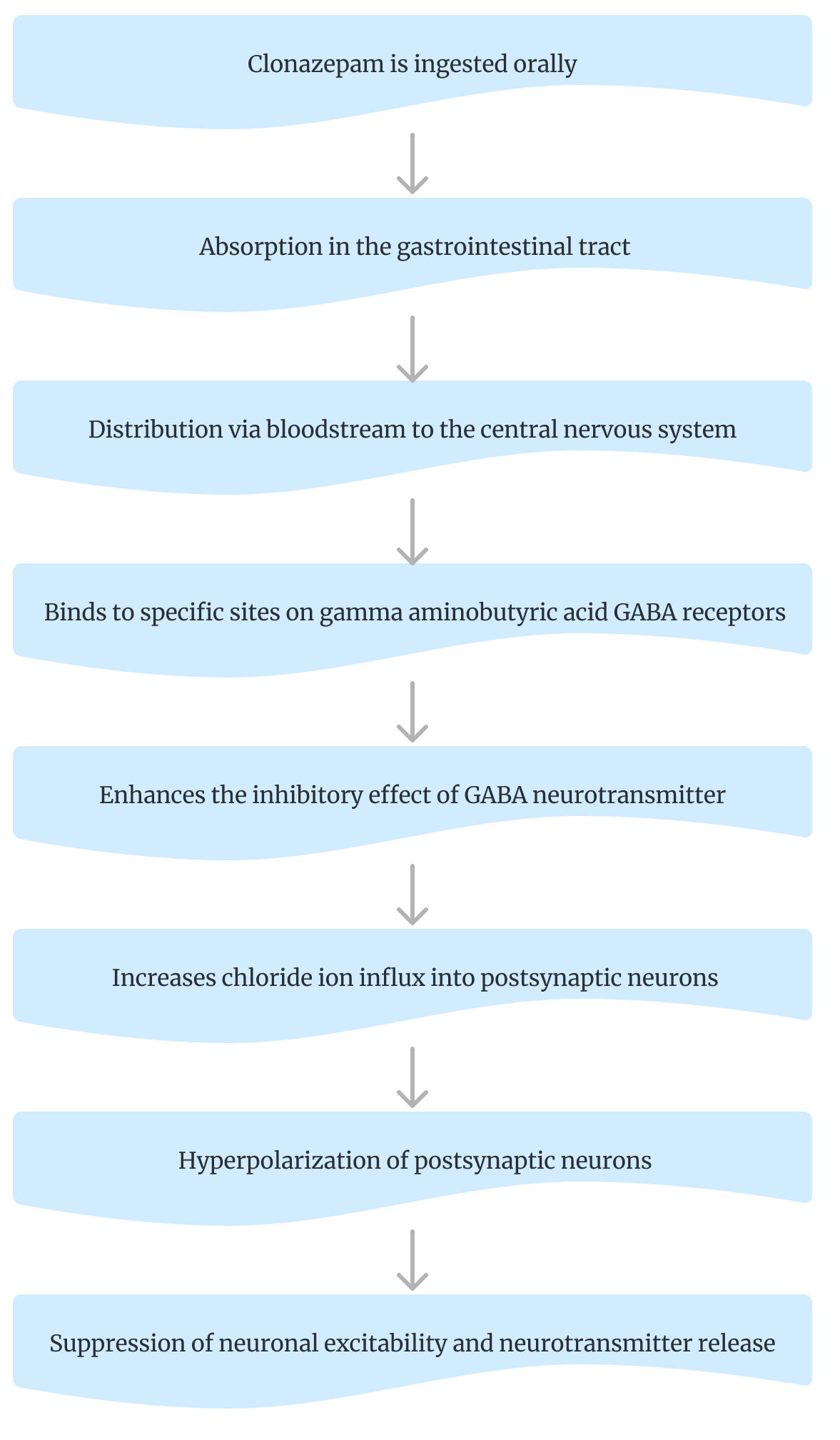
Figure 2. Mechanism of action of clonazepam |
Clonazepam, taken orally, is absorbed through the gastrointestinal tract into the bloodstream, then transported to the central nervous system. There, it binds to GABA receptors, enhancing GABA's inhibitory effect. This increases chloride ion influx, hyperpolarizing neurons and suppressing excitability and neurotransmitter release.
Psychotherapies
Emerging Treatments and Research in the Field
Deep Brain Stimulation (DBS) involves surgically implanting electrodes to regulate brain activity for severe, treatment-resistant OCD [53, 54]. Research is exploring the therapeutic potential of ketamine and psychedelics combined with therapy for OCD [55]. Transcranial Magnetic Stimulation (TMS) uses magnetic fields to modulate brain activity, being studied as a treatment for OCD [56, 57]. Pharmacological interventions targeting the glutamatergic system are under investigation for OCD treatment [58]. Mindfulness-Based Interventions like MBCT and MBSR are being studied to enhance OCD treatment by increasing self-awareness and reducing reactivity to obsessive thoughts [59, 60].
Assessment
Risk to others: People with OCD often grapple with intrusive thoughts related to violence or aggression, leading to distress. This may result in inappropriate protective measures. Evaluating risks to others includes considering potential neglect of dependents, both physically and emotionally, as the demands of OCD can overshadow caregiving responsibilities [71, 72].
Conclusion
Obsessive-Compulsive Disorder (OCD) impacts between 1% and 3% of humanity and has a big impact on people, families, and society. The disorder manifests in diverse ways, from fears of contamination to hoarding behaviors, highlighting its intricate nature. Factors contributing to OCD include genetic predisposition, environmental influences, neurotransmitter imbalances, and cognitive distortions. Furthermore, OCD often co-occurs with conditions like depression, anxiety, and eating disorders, adding complexity to diagnosis and treatment. The societal impact of OCD encompasses reduced productivity, strained relationships, and stigma, which can impede access to support services. Addressing OCD effectively requires comprehensive approaches that promote awareness, education, early intervention, and equitable access to evidence-based treatments, aiming to mitigate its effects and foster a more understanding and supportive environment for those affected. Pharmacological interventions, primarily SSRIs, and psychotherapy, particularly CBT with ERP, offer hope for individuals grappling with OCD. SSRIs aim to restore neurotransmitter balance, while CBT with ERP challenges distorted thinking and helps confront fears without compulsions, enabling individuals to regain control and lead fulfilling lives.
The future of treating obsessive-compulsive disorder (OCD) appears bright as advancements in therapeutic techniques continue to evolve. One such promising modality is Deep Brain Stimulation (DBS), which shows potential in addressing severe cases of OCD that have proven resistant to conventional treatments. Additionally, there is growing interest in psychedelic-assisted therapies, which offer novel approaches to alleviating OCD symptoms by exploring the therapeutic benefits of substances like psilocybin or MDMA under controlled settings. Furthermore, the advent of personalized medicine heralds a new era in OCD treatment, wherein interventions can be customized according to individual needs and genetic predispositions. This tailored approach holds the promise of enhancing treatment efficacy by addressing the specific biological and psychological factors contributing to each patient's condition.
The horizon of obsessive-compulsive disorder (OCD) treatment shines brightly as innovative modalities continues to emerge, offering renewed hope for individuals grappling with this challenging condition. Among these modalities, Deep Brain Stimulation (DBS) stands out as a beacon of promise, particularly for those afflicted with severe cases of OCD that have proven resistant to traditional treatment approaches DBS can bring much-needed relief where previous therapies have failed by carefully regulating neural activity and implanting electrodes in certain brain areas. Apart from DBS, there's an increasing interest in investigating the potential therapeutic advantages of psychedelic-assisted treatments for OCD. These unconventional treatments involve the controlled administration of substances such as psilocybin or MDMA, often in conjunction with psychotherapy sessions conducted within carefully controlled settings. This innovative approach presents a fresh perspective on symptom alleviation, potentially disrupting entrenched patterns of OCD behavior and cognition and opening up new avenues for long-term healing and recovery. Furthermore, the advent of personalized medicine represents a significant leap forward in the realm of OCD treatment. By tailoring treatment strategies to the unique needs and genetic profiles of each patient, personalized medicine offers the potential for more precise and effective interventions.
In essence, the convergence of these innovative modalities—DBS, psychedelic-assisted therapies, and personalized medicine—heralds a new era in OCD treatment. With continued research, exploration, and refinement of these approaches, we stand poised to unlock transformative breakthroughs that have the potential to transform the landscape of OCD treatment, offering new hope and possibilities for individuals living with this challenging condition.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: None