Pharmacophore an International Research Journal
Pulmonary embolism (PE) occurs when a clot blocks a pulmonary artery. The condition is potentially life-threatening. Identifying patients at risk allows early interventions to reduce mortality. Symptoms and signs are nonspecific and underdiagnosed. this study is aimed at assessing the clinical patterns of presentations and risk factors of acute PE. A cross-sectional hospital-based study was done in Alshaab Teaching Hospital from May to December 2019. Data was analyzed using SPSS. Clinical presentations seen in decreasing frequency included: dyspnea of gradual onset at 34.4 %, pleuritic chest pain at 29.5 %, cough at 27.9 %, hemoptysis at 14.8%, and lower limb swelling at 11.5%. The post-surgical intervention was the highest risk factor 27.9 % especially orthopedics surgery, followed by the post-delivery period and respiratory disease 14.8 %. Computer tomography scan was the most often used method to confirm the diagnosis and low molecular weight heparin was the main treatment used. The study concluded that the presence of multiple risk factors is common in acute PE. Symptoms may be mild and maintenance of a high level of suspicion is essential. The highest prevalence was between 41-60 years. Mostly seen among females, the Method of diagnosis is used in clinical probability and CTPA, trans thoracic Echocardiography, and Doppler ultrasound in the presence of obvious limb swelling. Therapeutic measures were according to the guidelines. Most were discharged and arranged for outpatient follow-up. early presentation can decreases morbidity and mortality and improves outcomes, to offer high-risk groups prophylactic measures and better quantification of risk factors.
Introduction
Acute pulmonary embolism is a common and sometimes fatal disease. The approach to the evaluation should be efficient and at the same time avoid the risks of unnecessary testing so that treatment can be initiated as quickly as possible to avoid potential morbidity and mortality [1].
To diagnose acute PE we need the integration of a detailed history, physical examination, laboratory testing, and appropriate imaging techniques. There is a wide variation of clinical presentation of PE from one patient to another. Dyspnea is the most frequent presenting symptom. A massive PE presents with severe dyspnea, cyanosis, or syncope, while a peripherally located smaller PE is indicated by the presence of pleuritic pain, cough, or hemoptysis [2]. Tachypnea is the most common sign on physical examination. Patients without underlying cardiopulmonary disease were noted to appear anxious but otherwise well compensated despite an anatomically large PE [3]. On the contrary, patients with massive PE may present with hypotension, cardiogenic shock, or cardiac arrest. Patients with sub-massive PE usually fit between these 2 extremes. Systolic blood pressure is preserved but they exhibit signs of right ventricular failure, which include tachycardia, distended neck veins, tricuspid regurgitation, and an accentuated sound of pulmonic closure (P2) [4].
Evidence-based literature supports the practice of determining the clinical pretest probability of PE before proceeding with the diagnostic tests. American College of Physicians recommends that validated clinical prediction rules be used to estimate the pretest probability of PE and to interpret test results. There are many scoring systems used e.g., Modified Wells, Geneva, simplified Charlotte score, and Pisa model [5].
The D-dimer assay, along with clinical decision rules (CDRs), like the Well’s criteria and revised Geneva score, are reliable and well-validated methods to exclude venous thromboembolism in visitors of outpatients and emergency rooms [6].
D-dimer levels rise with age and in hospitalised patients because of acute care settings and the presence of substantial co-morbidities. Therefore, there is little information available regarding the ability to rule out VTE in hospitalised patients based on a D-dimer assay, with or without CDRs. Age-adjusted D-dimer (AADD) is utilised for pulmonary embolism in conjunction with other risk assessment scores and has been well-validated in numerous studies over the past ten years [7].
Research has been conducted to determine the usefulness of pO2 and/or pCO2 in the diagnosis of PE. It was determined that pO2 and/or pCO2 are insufficiently specific or sensitive for PE. PE cannot be diagnosed or ruled out with ABG alone [8].
When evaluating the pulmonary artery pressure and visualising the right ventricle, echocardiography is typically beneficial. It has been suggested for the noninvasive identification of evidence of pulmonary hypertension and right ventricular enlargement at the bedside, including right ventricular enlargement or hypokinesis of the free wall. In the event that cardiac ultrasonography reveals right ventricular dysfunction, the diagnosis of acute massive or sub-massive pulmonary embolism is supported [9].
Computed tomography pulmonary angiography (CTPA) has become the modality of choice to diagnose PE as it provides a multiplanar view for the assessment of pulmonary vessels to the subsegmental levels. RV dysfunction and the extent of pulmonary artery (PA) obstruction at computed tomography (CT) are useful as prognostic parameters. Patients with RV dysfunction and PE have a high mortality rate, and because of this, RV dysfunction is considered a poor prognostic marker. [10].
Currently, the use of thrombolysis is recommended only in patients with massive pulmonary embolism. Moderate pulmonary embolism is a subgroup of pulmonary embolism, which is characterized by hemodynamic stability, right ventricular enlargement, hypokinesia, or elevation of biomarkers of right ventricular injury [11].
In low-risk patients, anticoagulation should be started without delay in high and intermediate clinical probability of PE while diagnostic tests are running, but thrombolysis is not indicated [12].
Real-life data from the Computerized Registry of Patients with Venous Thromboembolism (RIETE) study suggest only a few patients with pulmonary embolism at low risk of complications were treated at home or hospitalized for less than 5 days, and it is obvious that management of PE appeared quite variable in different countries [13].
General Objectives: To assess clinical signs, symptoms, and common risk factors of Pulmonary Embolism among adults who attended the study area during the study period.
Specific Objectives: To determine common triggering and risk factors of PE. To determine the clinical patterns of presentation of PE. To determine the distribution of age and sex among patients diagnosed with PE.
Study Design
Cross-sectional, Observational hospital-based study.
Study Area
Alshaab Teaching Hospital in Khartoum state (capital of Sudan)
Study Population and Sample Size
All cases in ER, Respiratory ICU. CCU and General ward were diagnosed with pulmonary embolism during the study period from May to December 2018.
Inclusion Criteria
all patients diagnosed with PE.
Data Collection Tools and Methods
During the study period from May to December 2018, we interviewed all patients presented to the emergency rooms, respiratory ICU, CCU, and the general ward in Alshaab Teaching Hospital who were confirmed to have PE. We used a predesigned questionnaire that included sociodemographic data about patients and questions to collect data related to the objective of the research clinical presentation details, investigations used to confirm the diagnosis, the risk factors of PE, and the treatment given to these patients. All the information about patients was filled in by the researchers after explaining the aims of the study and obtaining written consent from them.
Statistical Analysis
The collected data were entered and analyzed using the Statistical Package for the Social Science (SPSS Inc. Chicago, IL, USA) version 17 for Windows. Descriptive statistics were performed. Percentages were given for quantitative variables. The significance was determined using the Chi-square test. P-value was considered significant if P < 0.05.
Results and Discussion
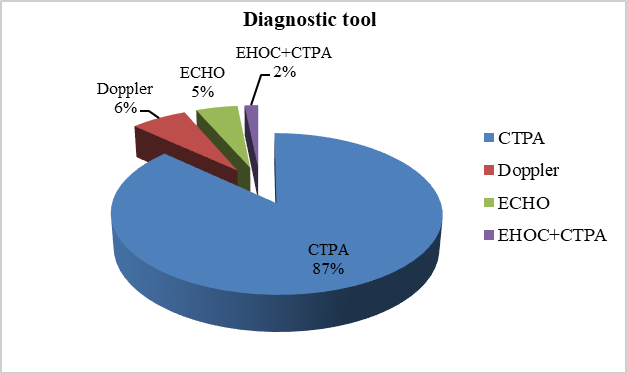
A total of sixty-one patients were enrolled in our study, the mean age was 55.83 with a standard deviation of 15.2. Regarding the method of diagnosis, all patients with a definitive diagnosis of Pulmonary Embolism included in the study were based on CTPA alone 53 (86.9%,), Doppler ultrasound plus clinical symptoms 4 (6.6%), and Echocardiography alone 3 (4.9%) as shown in Figure 1.
|
|
|
Figure 1. Distribution of the study population according to the diagnostic tool of PE |
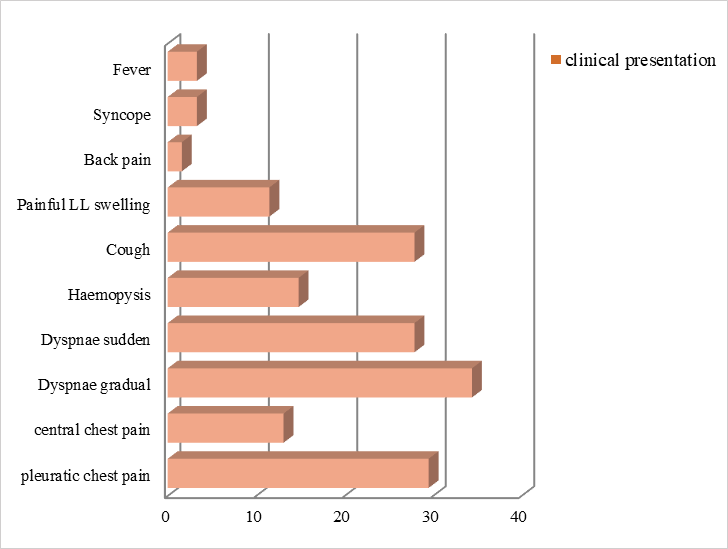
Common clinical presentation was found as follows: Patients presented with dyspnea were 38 (62.3%), 17 (27.9%) of dyspnea was of sudden onset and 21 (34.4%) was of gradual onset. Chest pain was the presentation in 27 (44.3%) patients, 18 (29.5%) of them had pleuritic chest pain and 9 (13.1%) had central chest pain. This is followed by hemoptysis in 9 (14.8%) patients, cough in 17 (27.9%) patients, Unilateral painful lower limb swelling in 7 (11.5%) patients, tachycardia in 11 (18%) patients, fainting and transient loss of consciousness in 2 (3.3%) patients and fever in 2 (3.3%) patients as shown in Figure 2.
|
|
|
Figure 2. Distribution of the study population according to the clinical presentations of PE |
The interval between the onset of symptoms and diagnosis was more than 24 hours in 98.4% of patients and only 1.6% presented in less than 24 hours.
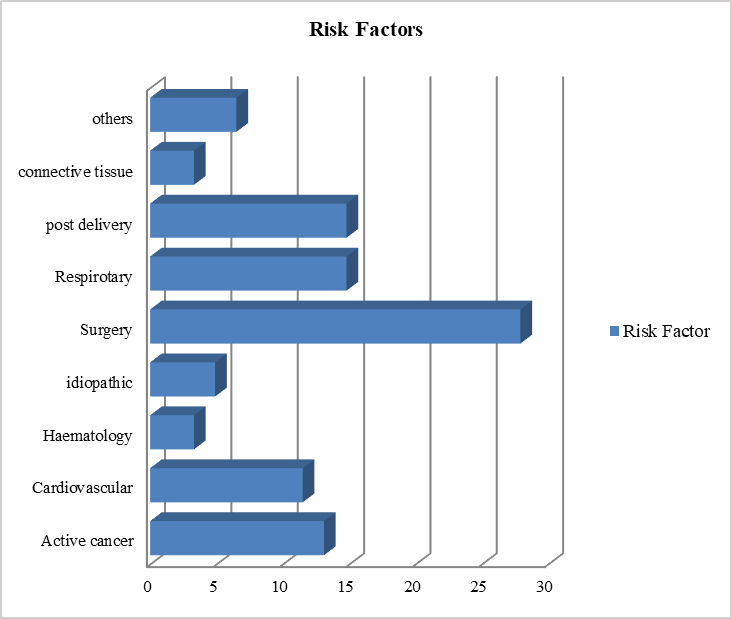
Regarding the risk factors of PE, most of the patients had one or more combined risks, the highest was among post-surgical procedures 17 (27.9%) with immobility for more than 4 weeks.
Post-delivery and puerperium period represented 9(14.8%). Active cancer patients on chemotherapy cycles or in palliative care represented 8(13.1%) as shown in Figure 3.
|
|
|
Figure 3. Distribution of the study population according to risk factors of PE |
The distribution of the study population according to the initial management of acute PE done in the hospital was as follows: 3 (4.9%) had Thrombolysis which was done in the coronary care unit and patients had cardiovascular risk factor. 2 (3.3%) received unfractionated heparin and 91.8% received Low Molecular Wight heparin and warfarin.
Regarding the outcome after admission, 57 (96.7%) were discharged and arranged for follow-up in the outpatient clinic and 2 (3.3%) died as shown in Table 1.
Table 1. Distribution of Outcome after admission of patients presented with PE (N=61).
|
The outcome |
The number/percentage |
|
discharged |
59 / 96.7% |
|
died |
2 / 3.3% |
Regarding patients taking prophylactic measures: post-surgical operation and post-delivery were 26 patients from a total of 61, only 7 (27%) had prophylaxis and 19 (73%) didn’t receive any prophylaxis as shown in Table 2.
Table 2. Distribution of patients with PE who received prophylaxis (N=61).
|
Prophylaxis |
The number/percentage |
|
Received prophylaxis |
7 / (27%) |
|
didn’t receive any prophylaxis |
19 / (73%) |
In this study, females were 39 (63.9 %), which is comparable to a study conducted in multi-center research from tertiary hospitals in Brazil [14], in which they found that 421 (57.9%) were females, and it is different from the finding in a Chinese study, in which they found that females were 46.8% [15]. More prevalent risk factors were seen in the age above 40 years (93.4%) in our study and also in the Chinese study. Neoplasm, pregnancy and postpartum, post-surgical operations, hip and lower limb fractures, and abdominal surgery were found as risk factors in our study and also it was the finding in many previous international studies [14, 15]. It is worth noting that no one was found to have stroke as a risk factor in our study as has been found in a previous study [16]. Congestive cardiac failure as a risk factor in our study represented 11.5% and this was also found in a case reported in 2021 [17]. Previous history of DVT/PE in the review study done by Morrone D and Morrone V [18] was a risk factor in 7 studies out of 8 this was also the finding in the study done by Hirmerova et al. [19] and it is found to be a risk factor in our study. Chronic respiratory disease and cor polmonale in our study comprise 14.8% of risk factors, this was the finding in a study done by Shapira-Rootman and his colleagues [20]. The commonest clinical presentation in our study was dyspnea which was the finding in 62.3% of participants, this was comparable to the Chinese study finding of 64.07%, but less than in the Brazilian study (78.4%) and also less than in Morrone and Morrone review (≥80%) in five studies out of eight [14, 18]. Chest Pain, cough, hemoptysis, and syncopal attack were found in 44.3%, 27.9 %, 14.8%, and 3.3% respectively in our patients, this was also found in previous international studies [21]. Fever was a presentation in 3.3% of our patients, in contrast to 11% and 22.14% for Brazilian and Chinese studies respectively [14, 15].
Most of the cases in our study were diagnosed using CTPA (86.9%), but venous duplex was done in 6.6% of patients, this is comparable to 87.7% and 2.4% in a previous study done by Warren and Matthews [22]. Heparins (unfractionated heparin and low molecular weight) were the most often used form of treatment in our study and in other centers around the world but in Sudan low molecular weight heparin (LMWH) is used more frequently than unfractionated heparin, 91.8%, and 9.2% respectively. Thrombolysis in this study was used in 4.9% of patients indicated to have high risk, this is the same indication for thrombolysis found in previous studies [23]. Other methods of treatment like Vena cava filter and embolectomy were not used by the participants in our study. Medical prophylactic measurements were not observed in this study in contrast to non -non-pharmacological prophylaxis (early mobility, elevation of the leg on pillows, pneumatic bed, and compression stockings) which was used in 11.4% of our patients. It is also observed that prophylactic measures were taken less frequently than recommended, which can lead to the development of PE. A detailed study regarding risk stratification of patients presenting with PE and the use of combined prophylactic measures and duration of use is needed especially post-operatively. Results of several international studies support extended prophylaxis after discharge in high-risk surgical patients and should be extended for at least 4 weeks in patients undergoing elective hip replacement and surgery for cancer [24, 25]. Prospective studies are required to assess the ideal period of antithrombotic therapy for thromboembolism in various types of surgery.
Conclusion
The presence of multiple risk factors is common in PE. There is a high or intermediate risk of minor symptoms. Objective clinical evaluation could point to the necessity of diagnostic research. High prevalence was seen in the age between 41-60 years, mostly seen in females. The most frequent clinical presentations seen were dyspnea of gradual onset and pleuritic chest pain. Less commonly seen presentations were fever and syncope which presented to the emergency room after more than 24 hours. The risk of PE was highest among post-surgical interventions followed by post-delivery and respiratory diseases. Methods of diagnosis should include clinical probability and CTPA, bedside echocardiography, and Doppler ultrasound in the presence of obvious limb swelling. The therapeutic measures used followed the international guidelines. Most of the patients were discharged and arranged for outpatient follow-up.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: Ethical approval was sought from the research directorate as the responsible authority in Alshaab Teaching Hospital and the ethical committee of the Sudan Medical Specialization Board. Written consent was obtained from all patients and to ensure confidentiality serial numbers were used instead of patient names.