Pharmacophore an International Research Journal
The outcome for newborns with respiratory distress syndrome has significantly improved since introducing surfactant therapy along with the initiation of bi-level positive airway pressure or continuous positive airway pressure. It has not been established yet regarding the best mode of respiratory assistance for pre-term neonates with respiratory distress syndrome. This investigation aims to evaluate the application of bilevel-positive airway pressure as a management approach for preterm newborns who have undergone surfactant therapy and compare it to other commonly used respiratory support methods. Our data suggests a positive trend towards a higher percentage of full-term births and a gradual decrease in preterm births over the evaluated period. This trend highlights notably the significance of surfactant therapy in the care of preterm infants. The use of CPAP has dropped tremendously, while the practice of BiPAP has shown a magnificent upsurge. Preterm newborns who received CPAP had higher levels of measured mean values of carbon dioxide compared to those treated with BIPAP. The lower carbon dioxide values in BIPAP-treated infants suggest that BIPAP may be a more effective form of respiratory support in maintaining proper carbon dioxide levels. In conclusion, the data analysis reveals a noticeable decrease in total newborns and the expansion of the use of BIPAP over CPAP for respiratory support. Our data suggests that BiPAP may be more effective in diminishing the necessity for intubation and the required time of ventilation for preterm newborns with respiratory issues.
Introduction
Premature newborns predominantly have respiratory distress syndrome (RDS), a respiratory condition. The outcome for these newborns has significantly improved since introducing surfactant therapy into the treatment regions. The initiation of bi-level positive airway pressure (Bi-pap) or continuous positive airway pressure (CPAP) plays an essential role in some newborns with RDS [1]. As a result, babies occurring before 32 weeks gestation have the largest risk of death, accounting for 47%, or an estimated 2.4 million, of all pediatric deaths, to occur in the newborn period. To narrow the disparity, the Sustainable Development Goals updated their targets in 2015 to bring newborn mortality down to 12 per 1,000 live births by 2030 [2].
It has not been established yet regarding the mode of respiratory assistance that is excellent for pre-term neonates with RDS. Comparatively, it is suggested that Bi-pap could be a more efficient type of respiratory support procedure for pre-term neonates than CPAP, as per the latest studies [3].
The principal objective of respiratory support is to inhibit and avoid hypoxemia and minimize the risk of associated complications. The most widely used techniques noninvasive ventilation (NIV) strategies, such as nasal continuous positive airway pressure (NCPAP) and nasal intermittent positive pressure ventilation (NIPPV), have been increasingly used as primary respiratory support in preterm infants with RDS. It has been proven through studies that in order to decrease the requirements for intubation, ventilation, and the frequency of broncho-pulmonary dysplasia, NIV is as efficient and efficacious as invasive mechanical ventilation (IMV) [4]. Besides, it operates without elevating the chances of detrimental events such as pneumothorax or mortality. Nevertheless, MIV is crucial in cases of failure of NIV to regulate sufficient gas exchange or if there are chances of severe apnea or acidosis occurrences. In addition to this, auxiliary respiratory assistance, such as high-frequency oscillatory ventilation (HFOV) or extracorporeal membrane oxygenation (ECMO) is essential for some pre-term infants who are more vulnerable to the adverse effects of RDS [5]. Those infants who stall conventional respiratory therapy are supported with these interventions. In conclusion, the introduction of surfactant administration and delivery of respiratory support is the most significant segment in the management of pre-term infants with RD [6]. The factors that determine the selection of the most suitable respiratory support modality are dependent on the graveness of the disease and the solitary requirements of the infant [1].
Introduction of bi-level positive airway pressure (bi-pap) as a potential solution Bi-level positive airway pressure (bi-pap) is the pre-eminent solution for those infants affected severely with RDS. This technique is suggested as a substitute respiratory support policy for premature infants with RDS who do not react well to NCPAP or those with a greater respiratory assistance requirement additional to NCPAP [7]. Recent studies suggest that bi-pap helps in reducing the obligation for invasive ventilation in comparison with other respiratory assistance techniques and may provide significantly improved outcomes [7, 8]. Bi-pap can result in great achievements including declined requirement for oxygen therapy, lower chance of bronchopulmonary dysplasia occurrence, and reduction in hospital stay. Whereas, as the amount of evidence and substantiation is restricted and disputable, some studies regarding this topic found no remarkable distinction in results between bi-pap and other modes of respiratory support [9-13].
The primary aim of this investigation is to evaluate the application of bilevel-positive airway pressure (BiPAP) as a management approach for preterm newborns who have undergone surfactant therapy. This investigation intends to assess the efficiency and safety of BiPAP as a respiratory assistance strategy in a specific population. To use a high degree of statistical significance, we analyzed the data from over five years from the year 2018 to 2022. Additionally, the analysis compares BiPAP to other commonly used respiratory support methods, Continuous Positive Airway Pressure (CPAP), targeting to provide valuable insights into the potential advantages and limitations in enhancing respiratory status. One of the objectives is to identify whether BiPAP delivers superior respiratory maintenance, reduces the requirement for mechanical ventilation, and results in better respiratory outcomes. It also aims to demonstrate the outcomes of newborns who received surfactant therapy. Moreover, the outcomes of this study may influence the treatment plans and choice of respiratory support for preterm newborns with respiratory distress.
Results and Discussion
The total number of newborns throughout 2018-2022 can be seen in Table 1. The year 2018 is the year with the highest number of newborns with 3806 newborns and the year 2022 is the year with the least number of newborns with 3322 newborns in that particular year. The year 2020 has the second least number of newborns with only 3435 newborns. This could be due to the global pandemic conditions, as most people were advised to stay home due to the pandemic influence on healthcare services and safety precautions. Many chose to give birth at home if there were no complications. The year 2021 saw a modest amount of increase in the number of newborns compared to 2020 but this increase was not sustained as the number dropped again in 2022. It can be observed a gradual decline in the number of newborns from 3806 in the year 2018 to 3322 in 2022, an average of 12% decrease in the total number of newborns. The trend indicates a slight decrease in the birth rates during these five years. Analyzing the birth trend is essential for healthcare professionals to comprehend the demographic changes as they might have implications for the population growth, age distribution, and overall socio-economic landscape. Additionally, it helps to design better healthcare for future mothers and infants.
Table 1. The total number of newborns over the period from 2018 to 2022
|
Year |
Total number of newborns |
|
2018 |
3806 |
|
2019 |
3549 |
|
2020 |
3435 |
|
2021 |
3502 |
|
2022 |
3322 |
In 2018, the percentage of male births was slightly lower than female births at 49.8% and 50.2% respectively. As we move to the year 2019, the male birth (1814) accounts for 51.1% of the total, while the female birth (1735) represents 48.9%. In the year 2020, the male birth (1759) percentage was 50.9% and female birth (1686) percentage was 49.1%. The male birth percentage in 2021 and 2022 was 50.2% and 50.7% respectively. Moreover, the female birth percentage is 49.8% and 49.3% in the years 2021 and 2022 respectively.
According to this particular data, the number of male newborns is slightly higher than that of female newborns except for the year 2018. However, it demonstrates a relatively balanced gender distribution with very slight variations in percentages from year to year. It is important to note that these statistics are limited to five years and one single center. This data is very crucial for assessing demographic trends and healthcare planning.
Table 2 explored a comparison between the total number of newborns vs preterm newborns from 2018 to 2022. The percentage of newborns who are born prematurely over the five years was 11.6%, 12.3%,10.8%,9.9% and 11% in 2018, 2019, 2020, 2021 and 2022 respectively. In 2019, there is a slim escalation in the percentage of preterm births as compared to the year 2018. However, there is a substantial decline in the preterm birth percentage in the years 2020 and 2021 at 10.8% and 9.9 percentage respectively. This can also be because some women chose to give birth at home because of the pandemic. Additionally, the percentage increased from 9.9% to 11% from the year 2021 to 2022. On the whole, our data suggests a positive trend towards a higher percentage of full-term births and a gradual decrease in preterm births over the given period. This implies advancements in healthcare and prenatal care contributing to better maternal and neonatal outcomes.
Table 2. The percentage of preterm newborns compared to the total newborns throughout 2018-2022
|
Year |
Total number of newborns |
Percentage of full-term newborns |
Preterm newborns |
Percentage of preterm newborns |
|
2018 |
3806 |
88.4% |
441 |
11.6% |
|
2019 |
3549 |
87.7% |
435 |
12.3% |
|
2020 |
3435 |
89.2% |
371 |
10.8% |
|
2021 |
3502 |
90.1% |
348 |
9.9% |
|
2022 |
3322 |
89% |
365 |
11% |
Table 3 reveals the number and proportion of preterm newborns who were treated with surfactants over the five years. The administration of surfactant therapy considerably increased from 7% in 2018 to 13.7% in 2022. This trend highlights notably the significance of surfactant therapy in the care of preterm infants while understanding the requirement of ongoing attempts to advance its accessibility and effectiveness.
Table 3. The proportion of preterm newborns and preterm newborns treated with surfactants over 2018-2022
|
Year |
Preterm newborns |
Percentage of preterm newborns without surfactant |
Preterm newborns treated with surfactant |
Percentage of preterm newborns treated with surfactant |
|
2018 |
441 |
93% |
31 |
7% |
|
2019 |
435 |
92% |
35 |
8% |
|
2020 |
371 |
90.6% |
35 |
9.4% |
|
2021 |
348 |
90.1% |
29 |
8.3% |
|
2022 |
365 |
89% |
50 |
13.7% |
All the newborns who received surfactant therapy were provided with CPAP. Throughout five years, from 2018-2022, despite the variations in the overall preterm birth rates, there was a consistent effort to provide surfactant treatment. As surfactant therapy plays a vital part in the enhancement of lung function and the overall survival of preterm newborns, it is significant to deliver surfactant to preterm newborns. Even though surfactant therapy is expensive, the hospital has a National Program that helps to fund the therapy plans.
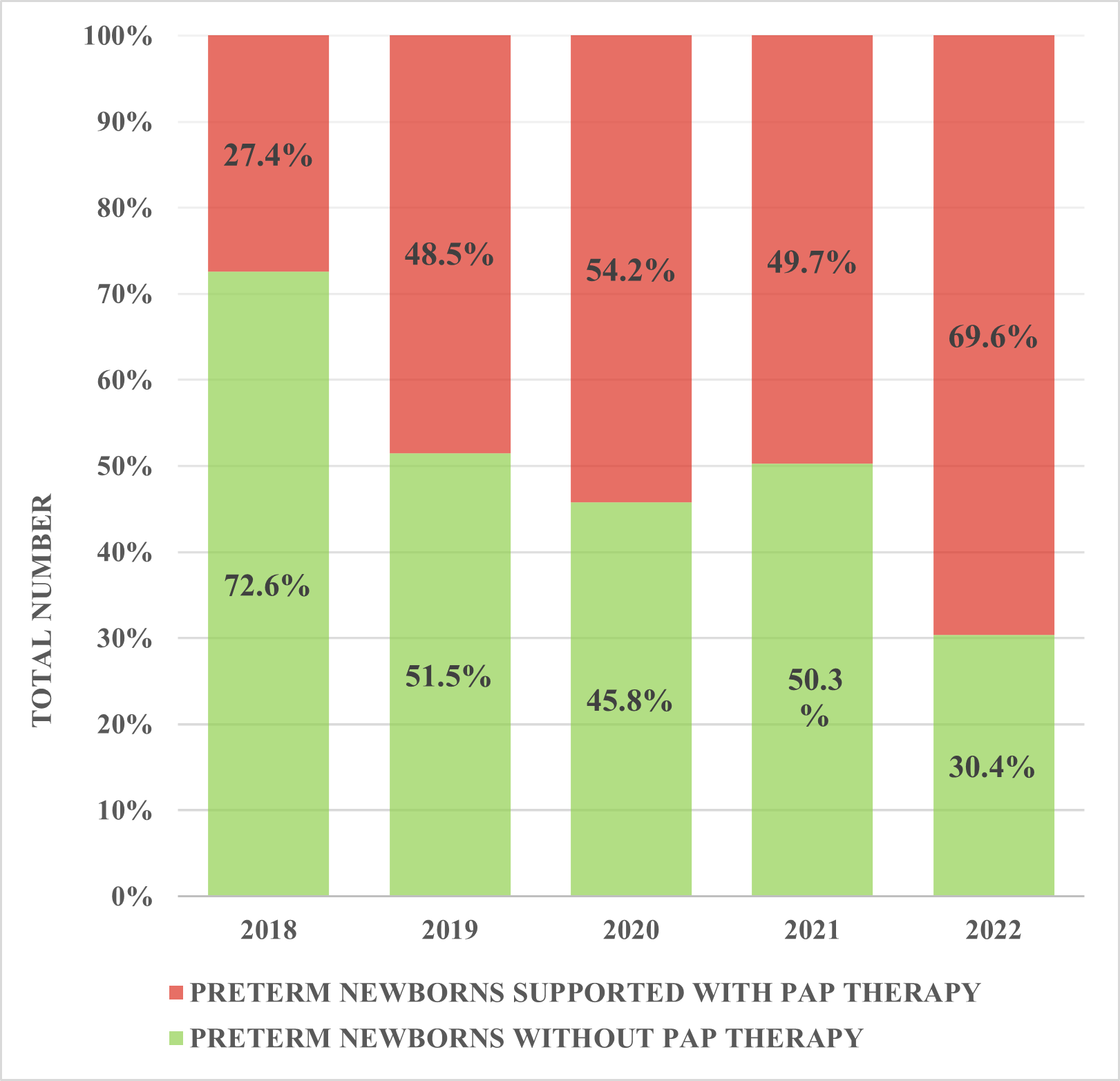
We evaluated the proportion of preterm newborns who received PAP therapy throughout 2018-2022. In the year 2018, 72.6% (320 cases) were not provided with PAP, and 27.4% of the infants (121 cases) were given PAP. However, in 2019 48.5% of the infants received PAP. The year 2020 witnessed a remarkable shift where the percentage of preterm newborns supported with PAP (54.2%) surpassed the percentage without PAP (45.8%) for the first time. The distribution in 2021 showed a slight increase in preterm newborns without PAP accounting for 175 cases (50.3%) while 173 infants (49.7%) received CPAP support.
The percentage of preterm newborns without PAP showed a declining trend which dropped from 72.6% in 2018 to 30.4% in 2022. Conversely, the PAP receiving preterm percentages showed a consistent upward trend peaking at 69.6% in 2022.
|
|
|
Figure 1. The proportion of newborns treated with PAP therapy 2018-2022 |
Figure 1 displays valuable insights into the changing trends in PAP utilization, highlighting the impact of this therapy in managing the respiratory challenges of preterm newborns. The graph presents a continuous enhancement in the overall care provided to preterm newborns with a larger proportion of them receiving PAP support over the years. Additionally, the advancements in medical technology and medical infrastructure have contributed to the changes.
The trend of the proportion of newborns treated with PAP therapy reveals a positive shift towards better healthcare practices with a vital increase in the percentage of preterm newborns who received the PAP. This positive trend implies a growing awareness and implementation of PAP as an effective intervention for supporting preterm infants with respiratory distress. This data underscores the importance of PAP as a life-saving intervention that can advance the health results for preterm newborns facing respiratory distress.
We evaluated the number of preterm newborns with different types of respiratory support over five years (2018-2022).
|
|
|
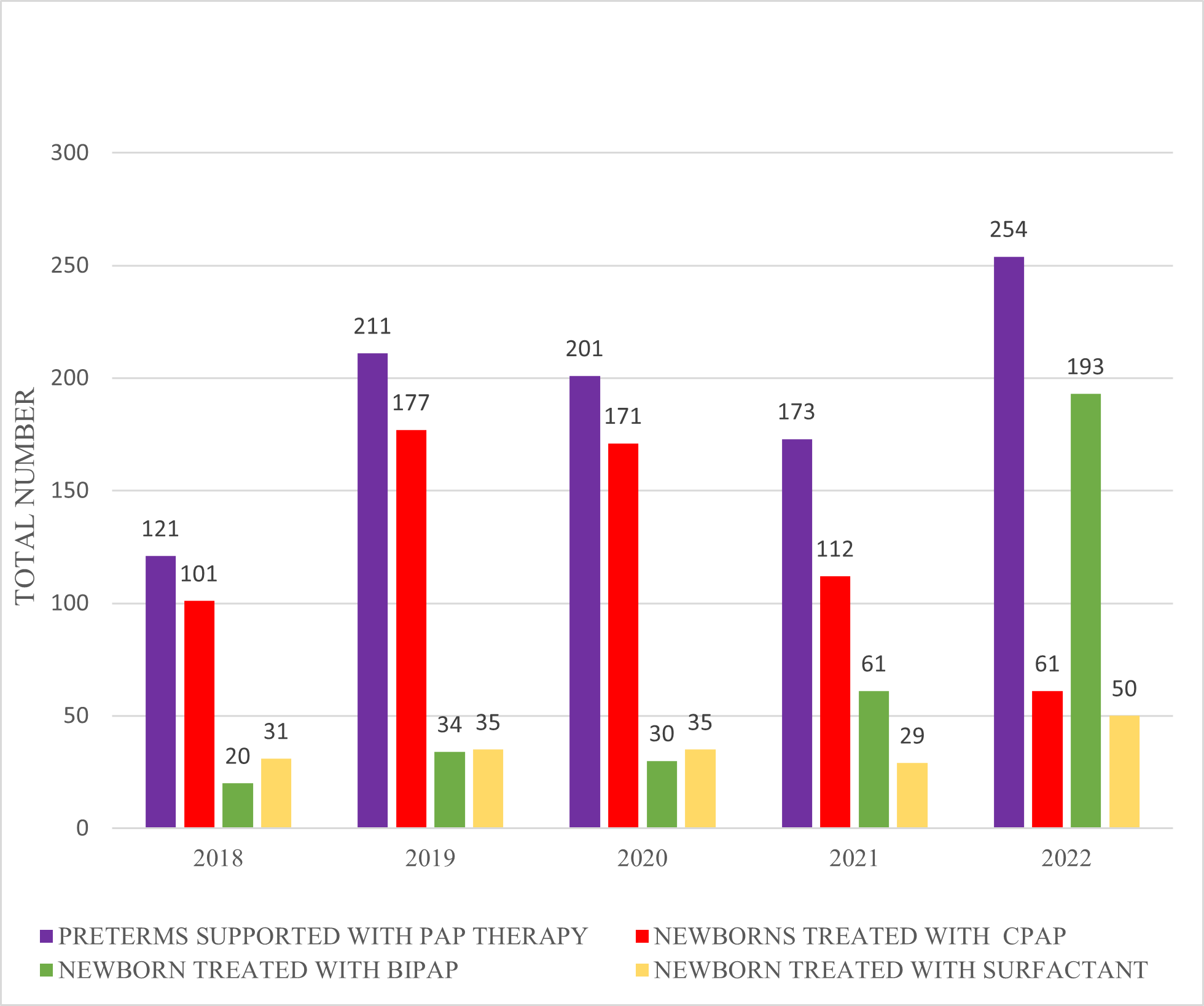
Figure 2. Preterm newborns with different types of respiratory support 2018-2022 |
The number of preterm newborns supported with PAP therapy varied each year with the highest number in 2022 at 254 and the lowest in 2018 at 121. It showed a positive shift over the five years. Among the preterm newborns receiving the PAP therapy, there was a varying distribution between CPAP and BiPAP treatments, with CPAP being more common in earlier years and BiPAP more customary in recent years with the year 2022 using BiPAP for 193 cases while CPAP was used only for 61 infants. Notably, the usage of surfactants has also increased over the five-year period, which rose from 31 cases in 2018 to 50 cases in 2022 signifying active efforts in increasing the usage of surfactants.
Overall, it shows an increasing trend in providing respiratory support over the years. However, the distribution between CPAP and BiPAP appears to have shifted over time demonstrating potential changes in clinical practices or advancements in technology. It highlights the trends and variations in these treatments delivering valuable insights into supporting preterm newborns with respiratory distress.
We compared the proportion of preterm newborns treated with CPAP and BiPAP from 2018 to 2022.
The number of preterm newborns supported with CPAP starts at 101 cases accounting for 83.5% of the total PAP therapy in 2018, which shows a slight increase to 177 cases in 2019. It is followed by a decline to 171 cases in 2020 and further drops to 112 cases in 2021. Finally, number of preterm newborns supported with CPAP continues its downward trend and stoops down to 61 cases, reaching 24% of the total PAP treatment in 2022.
The number of preterm newborns treated with BiPAP was 20 cases in 2018, goes up to 34 cases in 2019 and slights drops down to 30 cases in 2020. It depicts a noteworthy surge to 61 cases in 2021 and further shows a sweeping escalation to 193 cases, accounting for 76% of the entire PAP therapy cases in 2022. From the same Figure 2, it is evident that there has been a shift in the type of PAP therapy used over the five years. The use of CPAP has dropped tremendously from 83.5% in 2018 to 24% in 2022, while the practice of BiPAP has shown a magnificent upsurge from 16.5% in 2018 to 76% in 2022.
We compared the necessity for intubation despite being on different types of respiratory support for preterm newborns over the five years from 2018-2022 based on the two different forms of treatment CPAP and BiPAP.
|
|
|
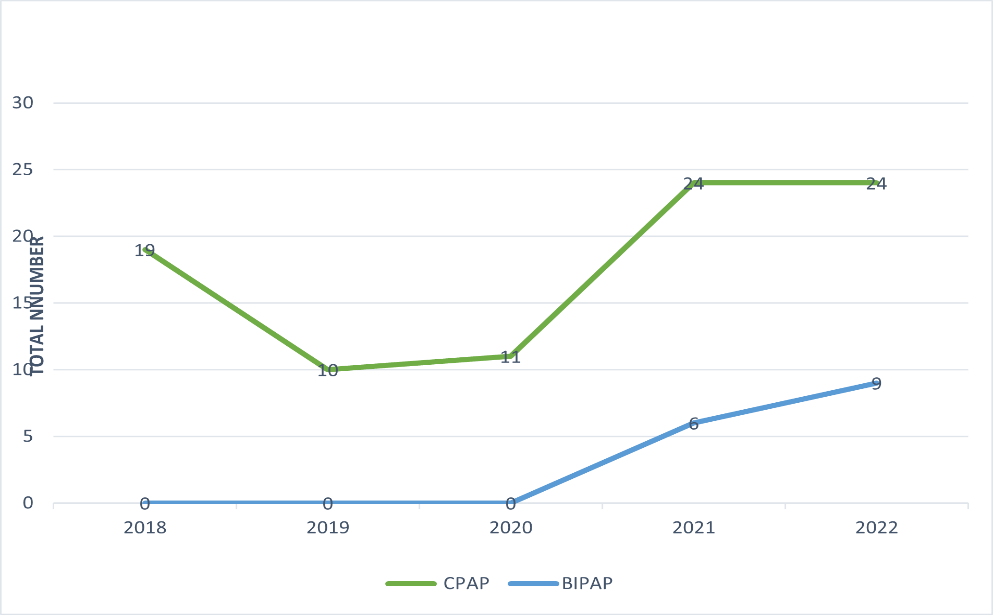
Figure 3. Comparison of the necessity of intubation for preterm newborns treated with CPAP and BiPAP 2018-2022 |
The treatment with CPAP started for 19 cases in 2018 and dropped down to 10 cases in 2019. Besides, it remains almost adjacently in the year 2020 at 11 cases. From 2018-2020, the necessity for intubation was 100% accounted for by the preterm newborns who received CPAP. The year 2021 shows a prominent surge to 24 cases and it maintains at same number of 24 cases in the following year 2022. However, in the years 2021 and 2022, the necessity for intubation in preterm who received CPAP accounted for 80% and 72.7% respectively.
The treatment with BiPAP indicated no preterm newborns were required for intubation who were treated with BiPAP in 2018, 2019, and 2020. In 2021, we observed an increase in the necessity for intubation which accounts for 20% of the total necessity of intubations. During 2022 witnessed a rise again to 9 cases which accounted for 27.3% of total cases. This can be due to a substantial increase in the number of preterm infants who were delivered with BiPAP.
Figure 3 depicted an increase in the number of cases with the necessity for intubation but the increase in practicing the supply of both CPAP and BiPAP has to be taken into consideration. In keeping with the data from the line graph, it is vital to note that the necessity for intubation is particularly decreased in the preterm newborns who were delivered BiPAP when taken in association with those who were delivered CPAP.
We compared the pH values as a mean in CPAP and BiPAP over the five years of 2018 to 2022.
The value of pH (mean) during CPAP treatment registered at 7.2 in 2018 and it lowered down to 7.13 in 2019. In the following year 2020, the mean pH rose to 7.26 and in 2021 it was 7.22, and in 2022, it further dropped to 7.20.
In patients treated with BiPAP, values of pH started at 7.26 and remained relatively stable in 2019 at 7.25 while during 2020 there is an elevation to 7.30. In the year 2021, it was 7.29 and it showed a prominent increase to 7.33 in 2022.
Taken as a whole, the pH levels for both treatments altered over the years but it appears to be a different trend for each of them. CPAP displays some variations with minute downward shifts while BiPAP demonstrates an overall positive trend in pH levels. These pH levels and trends are essential markers for assessing the effectiveness of the types of PAP therapy or monitoring the well-being of the preterm newborns to whom they are applied.
An increased value of pH designates an enhanced respiratory efficacy and better management of carbon dioxide in the body. According to the line graph, BiPAP has elevated pH values in comparison with CPAP which suggests that BiPAP is an improved respiratory support method.
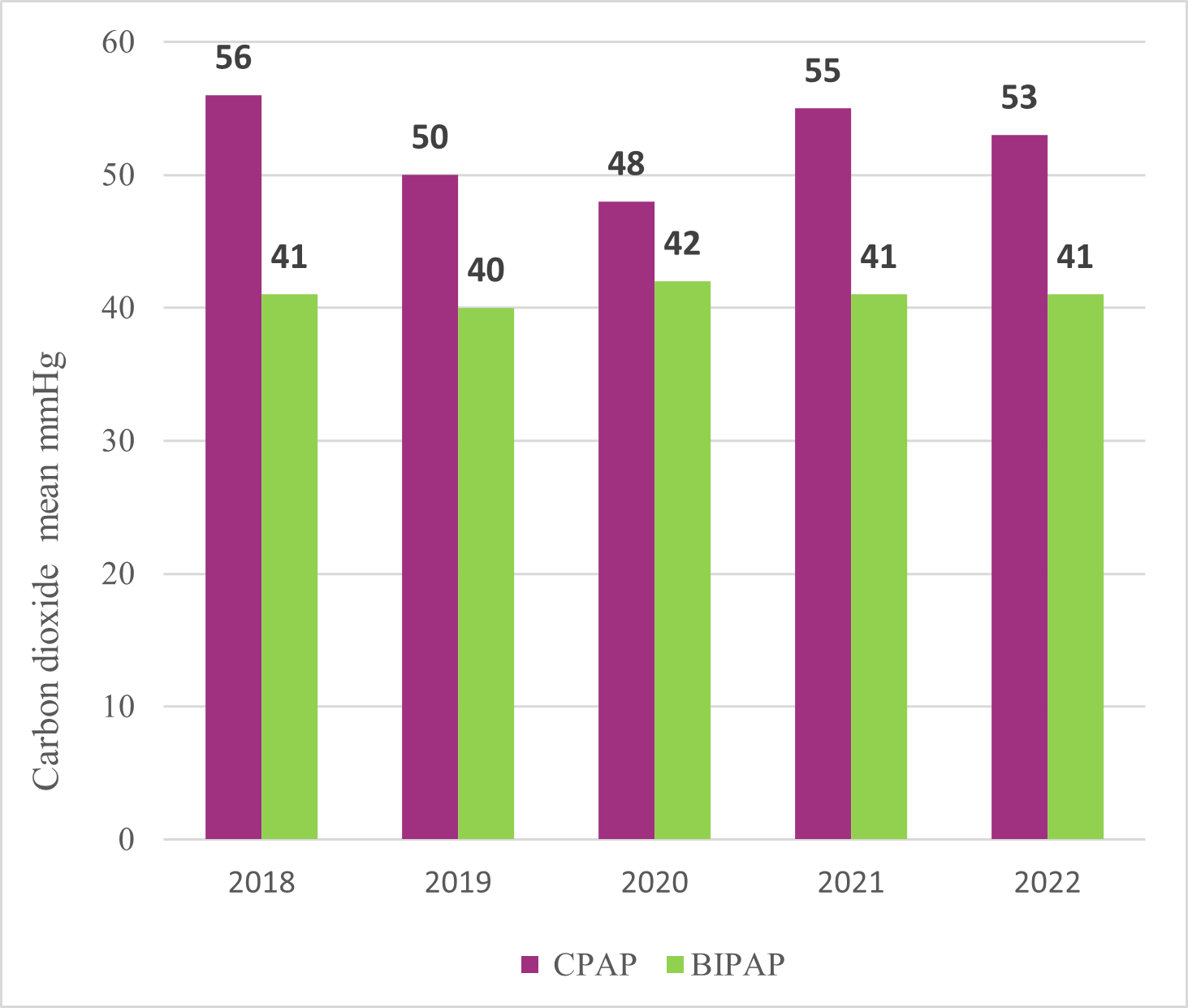
We evaluated in the same context the values of carbon dioxide expressed as mean mmHg provided in CPAP and BiPAP over the years 2018-2022 (Figure 4).
|
|
|
Figure 4. Carbon dioxide values provided in CPAP and BiPAP 2018-2022 |
In 2018, the mean carbon dioxide levels in preterm newborns who received CPAP were measured at 56 mmHg while those on BiPAP had a lower mean value of 41 mmHg. It implies that on average, CPAP patients had slightly higher values of dioxide in comparison with BiPAP during this year and it persisted through the years. In 2019, both CPAP (50 mmHg) and BiPAP (40 mmHg) showed a decline in mean carbon dioxide levels indicating betterment in both treatment methods. 2020 showed decreased carbon dioxide values to 48 mmHg and in 2021, carbon dioxide values in CPAP rose to 55 mmHg and it dropped again to 53 mmHg in 2022.
In general, the preterm newborns who received CPAP had higher levels of measured mean values of carbon dioxide. The average carbon dioxide values in the preterm newborns, maintained values between 40-42 mmHg throughout five years from 2018 to 2022. Lower dioxide values imply better respiratory efficacy and ventilation during therapy. It suggests that the treatment is successfully maintaining adequate air exchange and reducing the consequences of respiratory disturbances. Following the data from the graph, it is evident that BiPAP has lower dioxide values suggesting that it is the better form of respiratory support.
The data analysis reveals a noticeable falloff in the total number of newborns over the five years from 2018 to 2022, reflecting a downward trend within the represented region. There is an average of 12% decrease in total newborns over this period, just like the trend in the whole world.
Regarding gender distribution, according to the statistics, the number of male newborns was slightly higher than female newborns, except for the year 2018. However, the overall gender distribution remained relatively balanced with very slight variations in percentages from year to year. Our results indicate a positive trend towards a higher percentage of full-term births and a gradual decrease in preterm births. This implies that efforts to improve prenatal care and reduce preterm births have been effective [14, 15].
Furthermore, the consistent effort in providing surfactant treatment for preterm newborns over the five years demonstrates a commitment to enhancing neonatal care. Surfactant therapy is fundamental for the treatment of respiratory distress syndrome in preterm infants, and its consistent obtainability can significantly improve survival rates. Although prophylactic administration of surfactant was found to be significantly beneficial in reducing mortality and air leak in preterm infants in earlier trials without routine use of CPAP at birth, a systematic review that included two recent clinical trials requiring routine use of CPAP in the delivery room concluded that the benefit of prophylactic surfactant could no longer be demonstrated [16]. Instead, a concerning tendency toward higher mortality, bronchopulmonary dysplasia (BPD) at 28 days and 36 weeks, and BPD or death at 36 weeks was noted in this trial when prophylactic surfactant was used. Prophylactic surfactant usage was also linked to a significant rise in BPD, BPD, or mortality at 28 days, and a trend toward rising rates in the three trials when rates of prenatal corticosteroid exposure were high (>50%) [17, 18]. All of these can be complicated by difficult-to-manage infections [19, 20].
The evaluation of preterm newborns receiving positive airway pressure (PAP) support showcases a continuous enhancement in overall care. The larger proportion of preterm newborns receiving PAP support over the years indicates a positive response to the significance of respiratory support for premature infants. At the end of the follow-up, no newborns were receiving extra oxygen. No infants experienced nasal injuries or pneumothoraces, and no untoward events related to the trial were noted. The two devices' pressure-rate products were identical, but the breathing effort measured by the areas under the esophageal pressure-time curves showed that the Seattle-PAP required less breathing effort than the regular Bn-CPAP [21, 22].
Among the preterm newborns receiving PAP therapy, there has been a visible shift in the distribution between continuous positive airway pressure (CPAP) and bilevel positive airway pressure (BIPAP) treatments. CPAP was more frequently used in earlier years, while BIPAP became more customary in recent years. This trend may be indicative of evolving clinical practices or emerging evidence favoring BIPAP for certain cases [23].
Data about the necessity for intubation highlights a slight rise in the number of cases requiring intubation over the years but, the amplified usage of both CPAP and BIPAP therapies should be accounted for. The necessity for intubation is lower in preterm newborns who received BIPAP compared to those who received CPAP. This finding suggests that BIPAP might be a more effective respiratory support method, reducing the need for more invasive interventions like intubation [24]. In conclusion, both the CPAP and the BiPAP groups' rates of newborn reintubation within 72 hours of INSURE were similar. When it came to shorter (days) of PAP assistance and oxygen supplementation, BiPAP outperformed CPAP. The incidences of retinopathy of prematurity (ROP) and bronchopulmonary dysplasia (BPD) as well as lung function at one year of age did not differ between the two breathing techniques [25].
The analysis of pH levels indicates that BIPAP-treated preterm newborns exhibited higher pH values compared to CPAP-treated infants. This finding suggests that BIPAP might offer better respiratory support, possibly resulting in better acid-base balance for preterm newborns. Similarly, preterm newborns who received CPAP had higher levels of measured mean values of carbon dioxide compared to those treated with BIPAP. The lower carbon dioxide values in BIPAP-treated infants suggest that BIPAP may be a more effective form of respiratory support in maintaining proper carbon dioxide levels [26].
Conclusion
In conclusion, the data analysis reveals a noticeable decrease in total newborns over the five years with a relatively balanced gender distribution. Attempts to reduce preterm births and provide surfactant treatment were steadfast. The expansion of the use of BIPAP over CPAP for respiratory support advocates a potential shift in clinical practices. BiPAP demonstrated higher pH values and lower dioxide levels, indicating its potential as an upgraded respiratory support method. Additionally, the data suggests that BiPAP may be more effective in diminishing the necessity for intubation and the required time of ventilation for preterm newborns with respiratory issues. These findings emphasize the importance of continuous improvement in neonatal care to provide progressed outcomes for preterm infants.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the of Bihor County Emergency Clinical Hospital (241/06.03.2024).