Pharmacophore an International Research Journal
Polycystic ovary syndrome (PCOS) is a heterogeneous endocrinopathy characterized by oligo or anovulation, hyperandrogenism, and/or polycystic ovarian morphology. While women in both developed and developing nations are affected, it is also the leading cause of ovulatory infertility among women of reproductive age. This article discusses the epidemiology, risk factors, pathophysiology, diagnosis, and particular emphasis to its treatment. Global prevalence of PCOS ranges from 4 to 21% whereas it is between 9.1 and 36% among adolescents. Clinical presentation of PCOS can be mainly attributed to hyperandrogenism and chronic anovulation. Symptoms of hyperandrogenism include hirsutism, acne, and/or male pattern alopecia. Chronic anovulation proceeds with features such as oligomenorrhea, amenorrhea, and/or infertility. Even though a specific gene responsible is not found yet, it's clear that women with PCOS have two major genetic alterations involving androgen synthesis, insulin action, and also an increased incidence of other genetic alterations. Family history, obesity, and an unhealthy diet are found to be significant risk factors for the development of PCOS. The fundamental pathological changes in PCOS include hyperandrogenism, abnormality of gonadotropin secretion, and insulin resistance. It has been noted that genes, HAS2 & CBLN1 that are associated with ovulation are expressed less in granulosa cells of PCOS patients. These cells also show significantly differentially expressed genes for transcription factors and secretory proteins in addition to having increased Toll- & NOD-like receptors. Presently, there is no universal treatment for PCOS.
Introduction
Polycystic ovary syndrome (PCOS) is a heterogeneous endocrinopathy characterized by oligo/anovulation, hyperandrogenism, and/or polycystic ovarian morphology. Whilst androgen excess is a clinical hallmark of this condition, it can manifest either as a predominantly morphological or a biochemical syndrome [1]. Depending on the diagnostic criteria applied, the prevalence of PCOS varies from 4 to 21% worldwide and from 9.1 to 36% in teenagers. Additionally, it is the main factor causing ovulatory infertility in women who are of reproductive age [2].
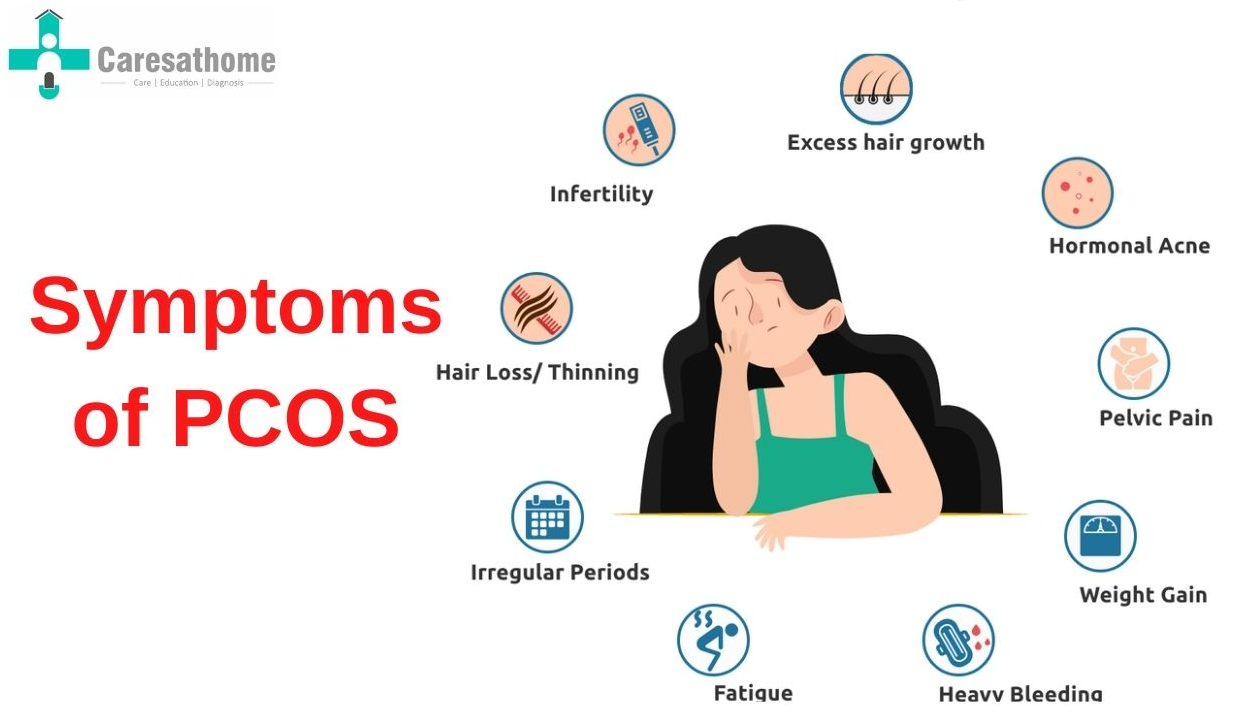
The clinical presentation of PCOS can be mainly attributed to hyperandrogenism and chronic anovulation. Symptoms of hyperandrogenism include hirsutism, acne, and/or male pattern alopecia (Figure 1). Chronic anovulation proceeds with features such as oligomenorrhea, amenorrhea, and/or infertility. Despite this, unaffected menstrual cycles could be seen in as many as 20% of PCOS patients [3]. Furthermore, it was also found that 50% of women with PCOS are obese [4]. In fact, oligomenorrhea and hyperandrogenism were more common in women with a history of weight increase, indicating that obesity may have a pathogenic role in the development of PCOS [5].
|
|
|
Figure 1. Symptoms of PCOS. (Image courtesy: Caresathome) |
Moreover, the disorder is not confined to reproductive function as metabolic function is also frequently compromised. According to a study, women with PCOS are associated with an increased risk for type 2 diabetes mellitus (T2DM), cardiovascular disease (CVD), dyslipidemia, hypertension, and glucose intolerance [6]. Although the exact etiology of PCOS is unknown, various theories have been proposed to explain its pathogenesis. Disruptions to the insulin axis, like hyperinsulinemia, are the basis of one idea. As a result, the liver's production of sex hormone-binding globulin (SHBG) is inhibited, which causes hyperandrogenemia [7]. Furthermore, hyperinsulinemia can also increase the frequency of gonadotropin-releasing hormone (GnRH) pulsations. As a result, luteinizing hormone (LH) is produced excessively so follicular maturation is decreased whereas ovarian androgen production is increased [8].
In this review, we address the current epidemiologic trends of PCOS and its pathophysiology, including risk factors. We also focus on the diagnostic criteria and explore various treatments and recommendations for women with PCOS.
Materials and Methods
The following databases were used to find research about current trends in PCOS for this narrative review: MEDLINE/PubMed, SCOPUS, Web of Science, ScienceDirect, NCBI, EBSCO, and Google Scholar. Initially, the search was conducted in Google Scholar using relevant Medical Subject Headings (MeSH) terms such as ‘PCOS’, ‘Treatment of PCOS’, ‘Biomarkers for PCOS’, etc. Afterward, the scope was widened to obtain more in-depth information. The same search process was also applied to other databases. Information was obtained from grey literature sources (CDC and RCOG) as well. The articles included were: (a) not restricted to a particular language but written in English (b) had an appropriate study design for the research question (c) historical accounts and recent cases; (e) original and peer-reviewed with a systematic approach. Articles were excluded based on the following criteria: (a) obsolete data; (b) insufficient or no data; (c) articles without a proper study or design approach; (d) articles that were out of scope; (e) articles with uncertainty in conclusion; (f) articles with unreliable/faulty statistical assessment; (g) articles with an uncertain source of data collection.
Epidemiology
The CDC defines epidemiology as the study of health-related states of events, including disease, and the application of this knowledge to the prevention and treatment of disease and other health issues [9]. Polycystic ovary syndrome (PCOS) is a complex endocrine disorder affecting 5-10 % of women of reproductive age. However, this can vary depending on the criteria used for diagnosis [10]. There are three main criteria used to diagnose PCOS. With the NIH/NICHD criteria, PCOS is indicated as a common endocrinopathy affecting 4-8% of the reproductive population of women. The prevalence of PCOS is two to three times greater than NIH/NICHD when the Rotterdam criteria is used and is approximately 15-20% [11].
Estimates place the prevalence of PCOS between 6% and 26% worldwide. a meta-analysis and systematic review of published research reporting PCOS prevalence based on at least one subset of diagnostic criteria. Depending on the parameters applied, their results showed that the prevalence of PCOS varies from 6% to 10% worldwide. Comparable epidemiological investigations found that the prevalence estimates from the Rotterdam and Androgen Excess Society were roughly double those derived using the National Institutes of Health's standards [12].
Numerous racial and ethnic groupings have high rates of PCOS. Women from North and South America, including those from Canada, Latinas, Africa, the Caribbean, Iceland, Europe, Southeast Asia, China, New Zealand, and the Middle East, exhibit different ethnic variances in the manifestation of the PCOS phenotype. Women of African descent with PCOS are more likely to have hypertension and CVD risk factors, whereas Hispanic women are more at risk for metabolic syndrome (MetS) and Type 2 Diabetes Mellitus (T2DM). Despite these phenotypic differences, there may not be significant differences in these reproductive or metabolic features in younger populations [13].
The close association between obesity and PCOS is supported by epidemiological data, revealing that between 38%-88% of women with PCOS are either overweight or obese. A meta-analysis of relevant studies reported in the literature showed that women with obesity had an odds ratio of 2.77 for the development of PCOS compared with their non-obese counterparts.
Homozygosity for the 5’-UTR variant is the most common in East Asian (32%) and Japanese (22%) populations and is less common among White (European and North American mainly (14%)) and Black (mainly African American (13%)) populations. However, these frequency estimates are likely to be affected by selection biases [14].
Risk Factors for PCOS
Genetics and Heredity Linkage
Even though a specific gene responsible has not been found yet, it is clear that women with PCOS have two major genetic alterations involving androgen synthesis, insulin action, and also an increased incidence of other genetic alterations.
Familial studies confirmed the heritability of PCOS and hyperandrogenemia. In a study with 115 sisters 80 women with PCOS were observed. 22% of these were fit for PCOS. Similar testosterone levels were seen between the sisters with just hyperandrogenemia and sisters and the probands who were observed as PCOS. A huge genetic component correlating with hyperandrogenemia was suggested and a bimodal distribution of testosterone level was observed in the sisters of women with PCOS.
Another study shows even the brothers of women with PCOS were observed with high levels of androgens. There have been studies that show an increased insulin secretion in PCOS patients due to insulin resistance. For example, a study conducted among the families of PCOS patients in Australia found that about 70% of all members of the family showed hyperinsulinemia [15].
A computational study for the genetic factors or proteins that are involved in PCOS has been done which showed that out of the 43 genes, that are involved in the steroidogenic pathways for the major steroid hormones, 14 significant genes were identified. From these genes, 8 genes were up-regulated while the other six genes were down-regulated. These 14 proteins are KTN1, CSRP2, CANX, CNN1, MPZL1, UBXN4, CYBRD1, MFAP4, NFYC, CD40, ANKFY1, SNAP23, NOTCH2, and WDR46 [16].
Even though several research has been carried out to find the causative genome for PCOS and positive results have been reported, there are no genes accepted as crucial to the etiology of PCOS. Although these studies support the role of genetic factors in the development of PCOS and phenotypic features, they tend to be less impactful. Despite this, multiple genes are used as biomarkers for the disorder.
Obesity, Lifestyle, and Insulin Action
Family history, obesity, and an unhealthy diet are found to be significant risk factors for the development of PCOS. Most of these factors are found to be interlinked with each other. The prevalence of PCOS in rural populations is less compared to those from urban areas. This could be due to a lack of awareness or unavailability of exposure to unhealthy foods, several types of pollution, and other causes of hormonal imbalance. The significant increase in obesity in urban areas might be the reason for the increased prevalence of PCOS in these areas. BMI is balanced by physical activity and a balanced diet. Moreover, Family history is also found to have the strongest association with PCOS [17].
Along with obesity, increased LH and decreased FSH levels are common presentations among women with PCOS. While it is a risk factor, the majority of obese women do not develop PCOS. This is because both androgen production and the clearance rate are increased together. However, in PCOS, the bioavailable androgen levels are increased, and this is further worsened by obesity as SHBG levels are reduced due to hyperinsulinemia. Apart from hyperandrogenism, PCOS also comes with GnRH, LH, and FSH level abnormalities [18]. Due to high testosterone levels, PCOS patients are likely to develop android obesity as well, where fat is deposited on the upper part of the body rather than the pelvic region i.e., gynecoid obesity. As a result, the femoral adipocytes are smaller in obese women with PCOS. Hence, this supports the hypothesis that visceral obesity is associated with hyperandrogenemia.
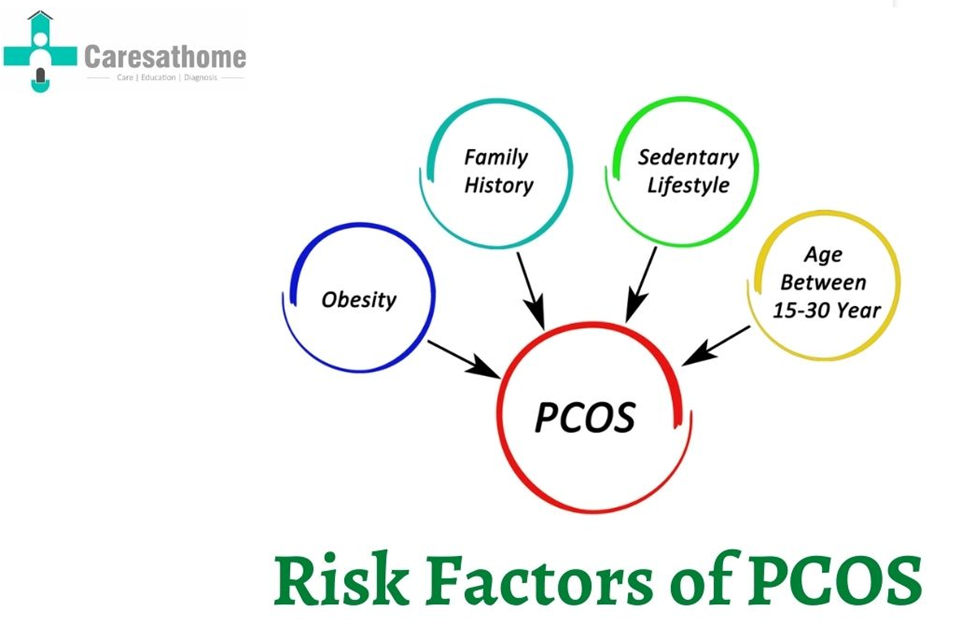
However, the link between PCOS and obesity is poorly understood. This could be because complications such as nonalcoholic fatty liver disease (NAFLD), hyperlipidemia, and insulin resistance can also be observed in both obese and non-obese women with PCOS. Furthermore, there is an underdiagnosis of PCOS in young girls. Since androgen excess manifests as hirsutism and other symptoms associated with hyperlipidemia or insulin resistance, the presence of PCOS can be masked starting from an early age [19]. Therefore, this is suggestive of testing even at young ages, especially in girls who have other numerous risk factors (Figure 2).
|
|
|
Figure 2. Risk factors for PCOS. (Image courtesy: Caresathome) |
Hyperandrogenism can also cause insulin resistance independent of obesity. This is due to a fault in the PI3-K post signaling pathway which can give rise to compensatory hyperinsulinemia. The hyperandrogenic and reproductive features of PCOS are driven primarily by the effects of compensatory hyperinsulinemia on the ovary. Conversely, the metabolic dysfunction and cardiometabolic risk that characterizes PCOS stems from a defective PI3-K post-receptor insulin pathway, the severity of which is influenced by body fat mass. Weight gain exacerbates the effect on metabolic, reproductive, androgenic secretions by separate pathways.
Congenital virilizing disorders, abnormal birth weight for gestational age, premature or exaggerated adrenarche, atypical sexual precocity, intractable obesity with acanthosis nigricans, metabolic syndrome, and pseudo-Cushing syndrome or pseudo-acromegaly in early childhood increase the risk of developing PCOS [20]. Environmental factors such as occupation, education, and cooking oil fumes influence the risk of PCOS as well. Additionally, obese, and overweight women have a higher risk of developing PCOS, but this can be reduced through lifestyle modifications [21].
Pathophysiology of Polycystic Ovary Syndrome
The fundamental pathological changes in PCOS include hyperandrogenism, abnormality of gonadotropin secretion, and insulin resistance. While no exact molecular mechanisms have been established for PCOS, we have studies that indicate relationships between genetics, epigenetics and the environment that can cause this multifactorial syndrome [22] (Figure 3). Some candidate loci of PCOS such as FSHR, LHCGR, INSR and DENND1A have been proposed to be forming a signaling network by which certain proteins and signaling cascades converge and regulate androgen synthesis in theca cells.
|
|
|
Figure 3. Pathogenesis of PCOS. (Image courtesy: The Nevada Center for Reproductive Medicine) |
It has also been indicated that an increase in expression of TUG1, a long non-coding RNA, may contribute to increased follicular activation and growth while also inhibiting the selection of a dominant follicle. This is due to the reduced cell proliferation, increased apoptosis, and autophagy in addition to increased aromatase expression and estradiol synthesis which are observed when TUG1 levels are low. Epigenetics, which is basically (reversible) changes in gene activity without changes in genotype that cause heritable phenotypic changes, have been indicated in PCOS as well. X chromosome inactivation, which is an epigenetic process, was shown to be skewed in a group of women with hyperandrogenic hirsutism. They also showed preferential expression of longer CAG repeats in the androgen receptor gene [23].
Diagnosis of PCOS
Biomarkers
A biomarker is a medical sign indicative of one’s medical state that is observable, measurable & reproducible. In the case of PCOS, multiple biomarkers have been noted to have an association with the pathology. These include genes, growth factors, hormones & altered metabolites [24].
Gene analysis has been conducted broadly to understand the mechanisms of PCOS and identify biomarkers for therapy & diagnosis. It has been noted that HAS2 & CBLN1 which are associated with ovulation are expressed less in granulosa cells of PCOS patients. These cells also show significantly different differentially expressed genes for transcription factors & secretory proteins in addition to having increased Toll- & NOD-like receptors [25].
TUG1 can also be used as a diagnostic tool as its levels are highly increased in PCOS patients. MicroRNAs could also be a potential biomarker as their altered expression is seen in patients with insulin resistance, infertility, atherosclerosis, lipid disorders & other disorders which have overlap with PCOS in clinical presentation. Certain growth factors can also be used as biomarkers. Serum levels of EREG & PDGF-D have been noted to be decreased in PCOS patients. Some cytokines used for PCOS screening include Irisin, Betatrophin, and Zinc-α2-glycoprotein (ZAG). They have better accuracy when an analysis is done for all three [26].
The hormones anti-Mullerian hormone (AMH) and testosterone are measured in the diagnosis of PCOS. AMH increases with ovarian follicles and cysts and therefore is useful for disease detection. Measuring serum testosterone along with sex hormone-binding globulin levels is used to assess hyperandrogenism. Hormones such as inhibin βA are also decreased in PCOS patients while the steroid hormone deoxycorticosterone was higher (in follicular fluid).
Metabolic syndrome and metabolic disturbances are common in PCOS patients. These effects could be reflected in the ovarian follicular fluid composition, where free fatty acids are increased while bioactive lipids are decreased. Phenylalanine and leucine levels are also increased. The use of metabolomics to identify more diagnostic markers for PCOS is an area of growing interest [27].
Criteria
National Institutes of Health (NIH)/National Institute of Child Health and Human Development (NICHD) criteria are hyperandrogenism, oligo/amenorrhea, and anovulation. European Society for Human Reproduction and Embryology (ESHRE)/ American Society for Reproductive Medicine criteria (ASRM)/ Rotterdam criteria is a previous criteria and ultrasound with evidence of multiple cysts around the ovary. Androgen Excess Society (AES) criteria is hyperandrogenism with ovarian dysfunction or cysts [28].
Management
Presently, there is no universal treatment for PCOS. Instead, it is symptom-oriented and tailored to the specific needs of each patient. In all situations, however, lifestyle counseling should be offered to prevent or treat obesity. As there are currently no medications approved for the treatment of PCOS, pharmacological therapy mainly focuses on managing hyperandrogenism, insulin resistance, and oligo-ovulation [29].
Lifestyle Recommendations
First-line treatment of PCOS includes lifestyle modifications such as dietary changes. Though an optimal diet is yet to be determined, it was recently found that a well-balanced diet composed of low protein, medium carbohydrate, and fat improved the reproductive outcome in mouse models of PCOS [30]. Similarly, aerobic exercises such as continuous aerobic exercise training (CAET) and high-intensity interval training (HIIT) have also been studied for their role in PCOS treatment. In 2021, a pilot trial was conducted to compare the effects of HIIT and CAET in women with PCOS. Despite the difficulties in studying their effects on ovulation, both CAET and HIIT have been reported to improve anthropometrics and several cardiometabolic health indicators [31].
For Hyperandrogenism in PCOS
For dermatological indications of hyperandrogenism, a combination of cosmetic techniques with topical and/or oral medication is frequently used. In the majority of these cases, oral contraceptive pills (OCPs) are needed for optimal outcomes [32]. Unfortunately, the use of OCPs also worsens the disease process and raises the risk of obesity, T2DM, and cardiovascular disease. Therefore, alternate therapeutic agents should be considered for high-risk patients.
In addition to OCPs, 5α-reductase inhibitors and androgen receptor blockers such as cyproterone acetate, spironolactone, or flutamide are included among the drugs of choice for hirsutism. While these drugs may also be used for severe cases of alopecia and acne, retinoids remain the gold standard against acne [33], whereas topical minoxidil was shown to be effective against alopecia.
For Insulin Resistance in PCOS
Metformin is the most commonly prescribed drug for insulin resistance, and it has similar advantages to lifestyle modifications [25]. Recent research shows that, however, glucagon-like peptide-1 (GLP-1) receptor agonist is more effective than metformin in increasing insulin sensitivity among PCOS patients [33]. Furthermore, a study with sodium-glucose co-transporter-2 (SGLT-2) inhibitors revealed promising results as a potential new therapeutic option.
For Oligo-Ovulation in PCOS
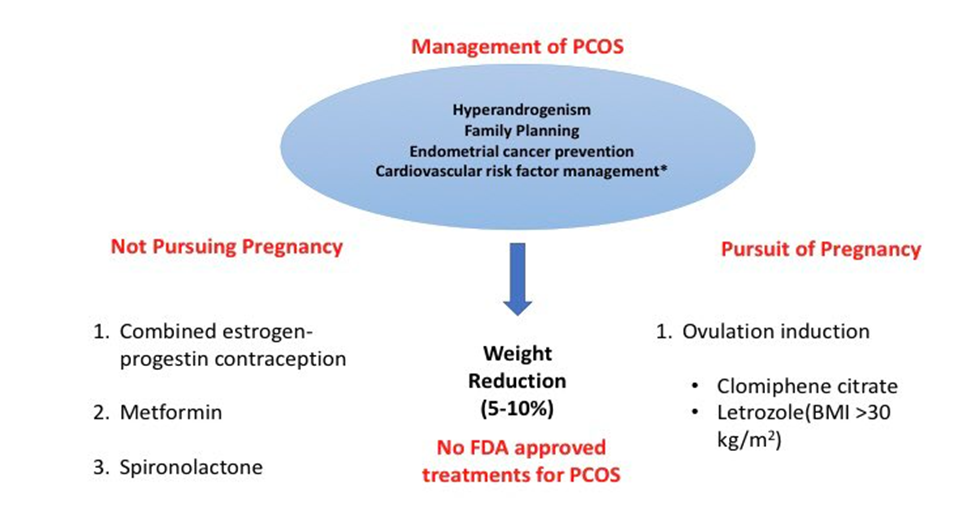
Treatment for oligo-ovulation must be tailored according to the patient's specific needs. In women who are not seeking immediate fertility, menstrual dysfunction may require specific interventions to prevent endometrial hyperplasia, if their menstrual bleeding occurs fewer than four times per year [34]. These interventions include OCPs and cyclic or continuous progestin treatment (Figure 4). If male factor infertility is also present, women who express a desire for fertility should be sent for assisted reproductive technology as soon as possible. For cases without male factor infertility, ovulation induction is included among first-line treatments, with clomiphene citrate or letrozole as the drugs of choice.
|
|
|
Figure 4. Treatment and management of PCOS: (Image courtesy: Dr. Gerald Diaz @GeraldMD, GrepMed Editor in Chief). |
Results and Discussion
PCOS is a heterogeneous endocrinopathy characterized by oligo/anovulation, hyperandrogenism, and/or polycystic ovarian morphology. The prevalence of PCOS varies from 4 to 21% worldwide and from 9.1 to 36% in teenagers. Additionally, it is the main factor causing ovulatory infertility in women who are of reproductive age. However, this can vary depending on the criteria used for diagnosis. There are three main criteria used to diagnose PCOS. With the NIH/NICHD criteria, PCOS is indicated as a common endocrinopathy affecting 4-8% of the reproductive population of women. The prevalence of PCOS is two to three times greater than NIH/NICHD when the Rotterdam criteria is used and is approximately 15-20%.
Depending on the parameters applied, their results showed that the prevalence of PCOS varies from 6% to 10% worldwide. Numerous racial and ethnic groupings have high rates of PCOS. Women from North and South America, including those from Canada, Latinas, Africa, the Caribbean, Iceland, Europe, Southeast Asia, China, New Zealand, and the Middle East, exhibit different ethnic variances in the manifestation of the PCOS phenotype [35]. Women of African descent with PCOS are more likely to have hypertension and CVD risk factors, whereas Hispanic women are more at risk for metabolic syndrome (MetS) and Type 2 Diabetes Mellitus (T2DM) [36]. Despite these phenotypic differences, there may not be significant differences in these reproductive or metabolic features in younger populations. The close association between obesity and PCOS is supported by epidemiological data, revealing that between 38%-88% of women with PCOS are either overweight or obese [37]. A meta-analysis of relevant studies reported in the literature showed that women with obesity had an odds ratio of 2.77 for the development of PCOS compared with their non-obese counterparts [38]. Even though a specific gene responsible has not been found yet, it is clear that women with PCOS have two major genetic alterations involving androgen synthesis, insulin action, and also an increased incidence of other genetic alterations. A huge genetic component correlating with hyperandrogenemia was suggested and a bimodal distribution of testosterone level was observed in the sisters of women with PCOS. Another study shows even the brothers of women with PCOS were observed with high levels of androgens [39]. There have been studies that show an increased insulin secretion in PCOS patients due to insulin resistance. For example, a study conducted among the families of PCOS patients in Australia found that about 70% of all members of the family showed hyperinsulinemia. A computational study for the genetic factors or proteins that are involved in PCOS has been done which showed that out of the 43 genes, that are involved in the steroidogenic pathways for the major steroid hormones, 14 significant genes were identified. From these genes, 8 genes were up-regulated while the other six genes were down-regulated [40]. These 14 proteins are KTN1, CSRP2, CANX, CNN1, MPZL1, UBXN4, CYBRD1, MFAP4, NFYC, CD40, ANKFY1, SNAP23, NOTCH2, and WDR46. Family history, obesity, and an unhealthy diet are found to be significant risk factors for the development of PCOS [41]. The fundamental pathological changes in PCOS include hyperandrogenism, abnormality of gonadotropin secretion, and insulin resistance. While no exact molecular mechanisms have been established for PCOS, we have studies that indicate relationships between genetics, epigenetics and the environment that can cause this multifactorial syndrome. Gene analysis has been conducted broadly to understand the mechanisms of PCOS and identify biomarkers for therapy & diagnosis [42]. It has been noted that HAS2 & CBLN1 which are associated with ovulation are expressed less in granulosa cells of PCOS patients. These cells also show significantly different differentially expressed genes for transcription factors & secretory proteins in addition to having increased Toll- & NOD-like receptors.
TUG1 can also be used as a diagnostic tool as its levels are highly increased in PCOS patients. MicroRNAs could also be a potential biomarker as their altered expression is seen in patients with insulin resistance, infertility, atherosclerosis, lipid disorders & other disorders which have overlap with PCOS in clinical presentation [43]. Presently, there is no universal treatment for PCOS. Instead, it is symptom-oriented and tailored to the specific needs of each patient. In all situations, however, lifestyle counseling should be offered to prevent or treat obesity [44]. First-line treatment of PCOS includes lifestyle modifications such as dietary changes. Though an optimal diet is yet to be determined, it was recently found that a well-balanced diet composed of low protein, medium carbohydrate, and fat improved the reproductive outcome in mouse models of PCOS [45]. In addition to OCPs, 5α-reductase inhibitors and androgen receptor blockers such as cyproterone acetate, spironolactone, or flutamide are included among the drugs of choice for hirsutism. Metformin is the most commonly prescribed drug for insulin resistance, and it has similar advantages to lifestyle modifications. Recent research shows that, however, glucagon-like peptide-1 (GLP-1) receptor agonist is more effective than metformin in increasing insulin sensitivity among PCOS patients. Treatment for oligo-ovulation must be tailored according to the patient's specific needs. In women who are not seeking immediate fertility, menstrual dysfunction may require specific interventions to prevent endometrial hyperplasia, if their menstrual bleeding occurs fewer than four times per year. These interventions include OCPs and cyclic or continuous progestin treatment.
Conclusion
Polycystic ovary syndrome (PCOS) is the leading cause of infertility in women, throughout the world. Obesity, food habits, lifestyle, inherited genes, hormones, and environment play a crucial role in the cause of PCOS. Among these factors, obesity and hormones are considered to be the leading role players for PCOS. Much research revealed after the drastic reduction of BMI, previously infertile due to PCOS became fertile and PCOS changed to normal. Due to the advent of medical technology polycystic ovary syndrome can be treated and managed considerably.
Acknowledgments: None
Conflict of interest: None
Financial support: None
Ethics statement: None